
記住我

Whether or not persons who have already been infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) should be vaccinated is unclear. Only a few studies have shown that vaccinees who were previously infected with SARS-CoV-2 had a significantly higher antibody response than previously uninfected vaccinees.1-4 In an observational cohort study, we enrolled 100 health care workers, including 38 (9 men and 29 women) with a documented history of SARS-CoV-2 infection (mean duration between infection and vaccination, 111 days). The mean age of these previously infected participants was 35.1 years (95% confidence interval [CI], 31.7 to 38.6). Our study also included 62 participants (25 men and 37 women) who had not been previously infected. The mean age of those participants was 44.7 years (95% CI, 41.0 to 47.6).
Both groups of participants received the messenger RNA vaccine BNT162b2 (Pfizer–BioNTech). Serum samples were obtained from the previously infected participants 10 days after the administration of the first dose and from the previously uninfected participants 10 days after the administration of the second dose. Thereafter, all the participants were screened for the presence of specific anti–SARS-CoV-2 spike IgG by means of a chemiluminescence microparticle immunoassay.
Figure 1. Figure 1. Immune Response in Participants with or without Previous SARS-CoV-2 Infection.
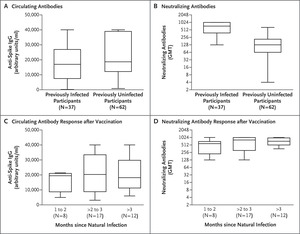
Figure 1. Immune Response in Participants with or without Previous SARS-CoV-2 Infection. Shown are titers of circulating severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) anti-spike IgG antibodies (Panel A) and neutralizing SARS-CoV-2 anti-spike IgG antibodies (Panel B) in serum samples obtained from previously infected participants after they received a single dose of vaccine and in samples obtained from previously uninfected participants after they received a second dose of vaccine. Differences in circulating (Panel C) and neutralizing (Panel D) IgG antibodies in samples obtained from previously infected participants were evaluated according to the duration from natural infection to vaccination (1 to 2 months, >2 months to 3 months, or >3 months). In each box-and-whisker plot, the horizontal line represents the median, the top and bottom of the box the interquartile range, and the whiskers the minimum and maximum values. GMT denotes geometric mean titer.
No significant difference in circulating anti-spike IgG antibody titers was observed between the samples from previously infected participants (mean level, 20,120 arbitrary units per milliliter; 95% CI, 16,400 to 23,800) and those from previously uninfected participants (mean level, 22,639 arbitrary units per milliliter; 95% CI, 19,400 to 25,900) (median levels are shown in Figure 1A). Circulating anti-spike IgG antibodies were not detected in only one previously infected participant; that participant did not have an antibody response to natural infection with SARS-CoV-2.
The same serum samples were also analyzed for the presence of specific anti–SARS-CoV-2 neutralizing antibodies. We observed a difference in levels of neutralizing antibodies between samples from the previously infected participants (geometric mean titer, 569; 95% CI, 467 to 670) and those from the previously uninfected participants (geometric mean titer, 118; 95% CI, 85 to 152) (P<0.001) (median levels are shown in Figure 1B). No substantial differences were noted between the titers from the previously infected and the previously uninfected participants according to age (Fig. S1 in the Supplementary Appendix, available with the full text of this letter at NEJM.org) or sex (data not shown).
The previously infected participants were categorized into three groups according to the time that had elapsed from infection to vaccination: 1 to 2 months (8 participants), more than 2 months to 3 months (17 participants), and more than 3 months (12 participants). The previously infected patient in whom circulating anti-spike IgG antibodies were not detected was not included in this categorization. The circulating IgG mean titers differed between the group vaccinated at 1 to 2 months and the group vaccinated at more than 2 months to 3 months after natural infection (mean level, 15,837 arbitrary units per milliliter [95% CI, 11,265 to 20,410] vs. 21,450 arbitrary units per milliliter [95% CI, 15,377 to 27,523]) (median levels are shown in Figure 1C); however, because the number of participants was limited, a real distinction cannot be made. No further significant difference was observed between the group of participants vaccinated at more than 2 months to 3 months and the group of those vaccinated more than 3 months after infection (mean level, 21,090 arbitrary units per milliliter [95% CI, 14,702 to 27,477]).
The differences among the three groups were more evident with respect to levels of neutralizing antibodies, with geometric mean titers ranging from 437 (95% CI, 231 to 643) in participants vaccinated 1 to 2 months after infection to 559 (95% CI, 389 to 730) in those vaccinated more than 2 months to 3 months after infection to 694 (95% CI, 565 to 823) in those vaccinated more than 3 months after infection (median levels are shown in Figure 1D). Although these findings indicate that the booster response was more efficacious when the vaccine was administered more than 3 months after infection, not enough information is available to draw a definitive conclusion.
The most remarkable finding of this study was the significantly lower neutralizing antibody titer after administration of a second dose of vaccine in previously uninfected patients than the titer after only a single dose of vaccine in previously infected participants. It is unclear how the neutralizing antibody titers influence the ability of the host to transmit the virus. These findings provide evidence that after the administration of a single dose of vaccine, the humoral response against SARS-CoV-2 in persons with a history of SARS-CoV-2 infection is greater than the response in previously uninfected participants who have received a second dose.
Gabriele Anichini, M.S.
Chiara Terrosi, M.S.
Claudia Gandolfo, Ph.D.
Gianni Gori Savellini, Ph.D.
University of Siena, Siena, Italy
Simonetta Fabrizi, M.D.
Giovanni B. Miceli, M.D.
Santa Maria alle Scotte University Hospital, Siena, Italy
M. Grazia Cusi, Ph.D.
University of Siena, Siena, Italy
[email protected]
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
This letter was published on April 14, 2021, at NEJM.org.
4 References1. Wise J. Covid-19: people who have had infection might only need one dose of mRNA vaccine. BMJ 2021;372:n308-n308.
2. Manisty C, Otter AD, Treibel TA, et al. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet 2021;397:1057-1058.
3. Saadat S, Tehrani ZR, Logue J, et al. Binding and neutralization antibody titers after a single vaccine dose in health care workers previously infected with SARS-CoV-2. JAMA 2021 March 1 (Epub ahead of print).
4. Krammer F, Srivastava K, Alshammary H, et al. Antibody responses in seropositive persons after a single dose of SARS-CoV-2 mRNA vaccine. N Engl J Med 2021;384:1372-1374.
留言 (0)