
記住我
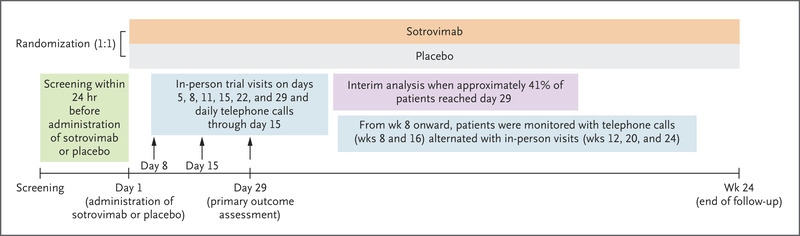


We conducted a global, randomized, placebo-controlled, phase 1–2–3 pivotal trial in which two 30-μg doses of BNT162b2 (Pfizer–BioNTech) were administered 21 days apart (ClinicalTrials.gov number, NCT04368728). These doses of vaccine had mainly low-grade side effects and provided 95% efficacy against coronavirus disease 2019 (Covid-19) from 7 days to approximately 2 months after dose 2.1 Efficacy waned to 84% between 4 and approximately 6 months after dose 2.2 Since vaccine authorization, viral variants have replaced the original strain, with the highly transmissible B.1.617.2 (delta) variant currently dominant.3 Although the effectiveness of the vaccine against severe disease, hospitalization, and death remains high, waning immunity and viral diversification create a possible need for a third vaccine dose.
Therefore, we administered a third 30-μg BNT162b2 dose 7.9 to 8.8 months after dose 2 to 11 participants 18 to 55 years of age and to 12 participants 65 to 85 years of age from U.S. sites in the phase 1 part of the ongoing pivotal trial (additional details of the trial are provided in Table S1 and text within the Supplementary Appendix, as well as in the trial protocol, both of which are available with the full text of this letter at NEJM.org). Local reactions and systemic events after dose 3 were predominantly mild to moderate and were similar to those after dose 2 (Figs. S1 and S2). No unsolicited adverse events were reported in the month after dose 3.
Figure 1. Figure 1. Neutralizing Responses after Two and Three Doses of BNT162b2.
Figure 1. Neutralizing Responses after Two and Three Doses of BNT162b2. The 50% neutralization titers against a wild-type target strain (USA-WA1/2020) and against B.1.351 (beta) lineage and B.1.617.2 (delta) lineage target strains are shown for both age groups. Geometric mean titers from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) plaque-reduction neutralization testing are shown for serum specimens obtained at the time points shown on the x axes from participants in the dose 3 immunogenicity population (11 participants in the 18-to-55-year age group and 12 participants in the 65-to-85-year age group). ? bars indicate 95% confidence intervals. Neutralization titers against wild-type virus were determined twice (once together with titers against each variant), and each titer against wild-type virus is reported separately with the corresponding variant titer. Differences among the determinations of the neutralization titer against wild-type virus represent experimental variation on repeat testing. Values above the error bars are geometric mean titers. Data points shown on the bar graph represent individual 50% neutralization titers. Individual titers for all participants are shown for all time points except for before dose 1, when all values were below the lower limit of quantitation (LLOQ) of 20; results below the LLOQ were set to 0.5 times the LLOQ. Geometric mean ratios (GMRs) of the titers against the variants and wild-type virus are shown below the graph. In Panel A, the geometric mean fold rises (GMFRs) in titers against the wild-type strain from before dose 3 to 1 month after dose 3 were 25.7 (95% confidence interval [CI], 12.4 to 53.3) for younger adults and 49.4 (95% CI, 29.2 to 83.3) for older adults. The corresponding GMFRs against the beta variant were 38.7 (95% CI, 19.8 to 75.5) and 78.3 (95% CI, 40.7 to 150.6), respectively.
We determined 50% serum neutralization titers against wild-type (USA-WA1/2020) severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and a recombinant beta variant strain (i.e., the beta variant spike gene on wild-type genetic background), as described previously.4 Serum specimens were obtained before dose 1, at 7 days and 1 month after dose 2, and before and 7 days and 1 month after dose 3 (Figure 1A). These data supported four key conclusions. First, during the approximately 8 months from 7 days after dose 2 to before dose 3, SARS-CoV-2 neutralization geometric mean titers (GMTs) in this subgroup of participants from phase 1 of the trial declined far more rapidly than vaccine efficacy declined in participants in the phase 2–3 pivotal trial.2 Second, by 1 month after dose 3, neutralization GMTs against wild-type virus increased to more than 5 times as high (in 18-to-55-year-olds) and to more than 7 times as high (in 65-to-85-year-olds) as the GMTs 1 month after dose 2. Third, neutralization GMTs against the beta variant increased more after dose 3 than did GMTs against wild-type virus, to more than 15 times as high (in younger adults) and more than 20 times as high (in older adults) as those after dose 2, reducing the gap between neutralization of wild-type virus and the beta variant. Fourth, neutralization GMTs decreased from 7 days to 1 month after dose 2 but increased from 7 days to 1 month after dose 3. A similar pattern of broader neutralization (i.e., against variant strains) and higher GMTs after dose 3 was seen in assays of neutralization GMTs against recombinant virus with delta variant spike protein on a wild-type genetic background: the geometric mean ratio of neutralization GMTs (delta variant to wild type) 1 month after dose 3 was 0.85 in younger adults and 0.92 in older adults (Figure 1B).
Increases in the magnitude and breadth of neutralization and improvements in the kinetics of the humoral response have also been observed with booster doses of prepandemic influenza vaccine administered after a primary immunization series.5 The safety and immunogenicity of a booster dose of BNT162b2 administered 7 to 9 months after the primary two-dose series suggest that a third dose could prolong protection and further increase the breadth of protection.
Ann R. Falsey, M.D.
University of Rochester, Rochester, NY
Robert W. Frenck, Jr., M.D.
Cincinnati Children’s Hospital, Cincinnati, OH
Edward E. Walsh, M.D.
University of Rochester, Rochester, NY
Nicholas Kitchin, M.D.
Pfizer Vaccine Research and Development, Hurley, United Kingdom
[email protected]
Judith Absalon, M.D.
Alejandra Gurtman, M.D.
Pfizer Vaccine Research and Development, Pearl River, NY
Stephen Lockhart, D.M.
Ruth Bailey, B.Sc.
Pfizer Vaccine Research and Development, Hurley, United Kingdom
Kena A. Swanson, Ph.D.
Pfizer Vaccine Research and Development, Pearl River, NY
Xia Xu, Ph.D.
Pfizer Vaccine Research and Development, Collegeville, PA
Kenneth Koury, Ph.D.
Warren Kalina, Ph.D.
David Cooper, Ph.D.
Pfizer Vaccine Research and Development, Pearl River, NY
Jing Zou, Ph.D.
Xuping Xie, Ph.D.
Hongjie Xia, Ph.D.
University of Texas Medical Branch, Galveston, TX
Özlem Türeci, M.D.
Eleni Lagkadinou, M.D., Ph.D.
BioNTech, Mainz, Germany
Kristin R. Tompkins, B.Sc.
Pfizer Vaccine Research and Development, Pearl River, NY
Pei-Yong Shi, Ph.D.
University of Texas Medical Branch, Galveston, TX
Kathrin U. Jansen, Ph.D.
Pfizer Vaccine Research and Development, Pearl River, NY
Uğur Şahin, M.D.
BioNTech, Mainz, Germany
Philip R. Dormitzer, M.D., Ph.D.
William C. Gruber, M.D.
Pfizer Vaccine Research and Development, Pearl River, NY
Supported by Pfizer and BioNTech.
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
This letter was published on September 15, 2021, at NEJM.org.
On request, and subject to certain criteria, conditions, and exceptions (see https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information), Pfizer will provide access to individual deidentified participant data from Pfizer-sponsored global interventional clinical studies conducted for medicines, vaccines, and medical devices for indications that have been approved in the United States or European Union or in programs that have been terminated (i.e., development for all indications has been discontinued). Pfizer will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data may be requested from Pfizer trials 24 months after trial completion. The deidentified participant data will be made available to researchers whose proposals meet the research criteria and other conditions, and for which an exception does not apply, through a secure portal. To gain access, data requestors must enter into a data access agreement with Pfizer.
5 References1. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med 2020;383:2603-2615.
2. Thomas SJ, Moreira ED Jr, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine through 6 months. N Engl J Med. DOI: 10.1056/NEJMoa2110345
3. Centers for Disease Control and Prevention. COVID data tracker. 2021 (https://covid.cdc.gov/covid-data-tracker/#datatracker-home).
4. Liu Y, Liu J, Xia H, et al. Neutralizing activity of BNT162b2-elicited serum. N Engl J Med 2021;384:1466-1468.
5. Galli G, Hancock K, Hoschler K, et al. Fast rise of broadly cross-reactive antibodies after boosting long-lived human memory B cells primed by an MF59 adjuvanted prepandemic vaccine. Proc Natl Acad Sci U S A 2009;106:7962-7967.
留言 (0)