The main findings of the current analysis can be summarized as follows (Graphical Abstract). First, most patients with very-high CV risk in the primary prevention setting are misclassified and their risk is underestimated. In fact, in 37% of cases, CV physician-perceived CV risk was underestimated, and only in 59.6% of cases there was proper risk stratification based on clinical judgment. This was confirmed by Cohen’s Kappa statistic that indicated poor agreement between perceived risk and calculated CV risk using validated tools. Second, patients whose risk is underestimated achieved less often the recommended LDL-C target and were less treated with lipid-lowering therapy. Third, in the multivariate analysis, underestimation of CV risk emerged as a significant negative predictor of achieving the LDL-C target, resulting in a half chance of achieving it.
The present study demonstrates a significant discrepancy between physician-perceived CV risk and the risk calculated using standardized scoring systems. Our findings reveal a significant underestimation of very-high risk patients, often categorized as high-risk based on clinical judgment. This misclassification is evident in the low measure of agreement between perceived and calculated risk, as indicated by a Cohen’s Kappa statistic of 0.208, suggesting only slight agreement. In primary prevention practice, physicians may rely too often on their own experience and intuition rather than formal risk assessment tools. This can lead to a subjective bias, where patients who do not outwardly exhibit severe symptoms may be perceived as low risk [10, 11]. In busy clinical settings, the time required to perform detailed risk assessments using tools like SCORE2 or SCORE2 OP may be seen as impractical. Consequently, quick judgments based on superficial assessments can prevail. Studies have shown that time pressure significantly influences clinical decision-making, leading to a reliance on heuristics and rapid assessments rather than thorough evaluations. This can compromise adherence to clinical guidelines and the thoroughness of patient care [12]. Most of the studies have focused on the gap in patients’ perception of their CV risk, rather than on misclassification by the physician. Grauman et al.[13] showed that individuals with very good general health (OR 2.60, 95% CI 1.10–6.16) and no family history of myocardial infarction (OR 2.27, 95% CI 1.24–4.18) are significantly more likely to underestimate their CV risk, with an especially pronounced effect among those with a high calculated risk (without family history OR 22.57, 95% CI 6.17–82.54; with very good/excellent health OR 15.78, 95% CI 3.73–66.87)[13]. This underestimation, influenced by a false sense of security due to perceived good health, can hinder the effective prevention and management of CVD. Navar et al.[14] examined the gap between patient-perceived and actual 10-year atherosclerotic CVD risk and its effect on willingness for preventive therapy in 4187 patients. There was no correlation between perceived and calculated risk (ρ=−0.01, p = 0.46), with 72.2% of patients overestimating their risk (mean perceived 33.3% vs. mean calculated 17.1%, p < 0.01). Patients had an overly optimistic view of their risk relative to peers. This misperception influenced willingness for future prevention therapy (p < 0.01) but not current statin use (p = 0.18). The perceived relative risk increased statin use (risk ratio 1.04 [95% CI, 1.02–1.06]) and willingness for prevention therapy (risk ratio 1.11, 95% CI 1.07–1.16) [14].
The implications of misalignment between physicians’ perception and calculated risk are profound. Underestimation of CV risk can lead to insufficient preventive measures and therapeutic interventions, potentially worsening patient prognosis. Conversely, overestimation may lead to unnecessary treatments, exposing patients to unwarranted side effects and increased healthcare costs. The underestimation of CV risk by clinicians may have critical implications for patient management, particularly in the implementation of aggressive lipid-lowering strategies. Our data indicate that 37% of patients were underestimated regarding their CV risk, while only 3.3% were overestimated. This discrepancy underscores a potential gap in clinical practice, where reliance on clinical judgment alone may not suffice for accurate risk stratification. Notably, only 16% of patients whose CV risk was underestimated reached their LDL-C target, compared to 34.5% in the well-estimated group and 76.9% in the overestimated group. This underachievement among underestimated patients correlates with a lower prescription rate of statins (29.2%) and statin/ezetimibe combination therapy (11.8%), compared to well-estimated patients (50% and 43.5%, respectively) and overestimated patients (76.9% for both therapies). Given that underestimation of risk was independently associated with a 47% lower likelihood of reaching LDL-C targets, it is imperative to enhance the accuracy of risk assessment tools utilized in clinical settings. Multivariate logistic regression analysis identified the use of statins, statin/ezetimibe combination, and bempedoic acid as significant positive predictors for achieving LDL-C targets. This finding aligns with existing literature that emphasizes the efficacy of these agents in lipid management and CV risk reduction [15]. Patients whose CV risk was overestimated were more likely to achieve the LDL-C target (OR 5.33, CI 1.33–21.42, p = 0.018), suggesting that a conservative approach to risk estimation may inadvertently benefit patient outcomes by prompting more aggressive treatment measures.
Regarding the control of LDL-C in primary prevention, the EURIKA study, which included patients with at least one major CV risk factor, found that only 41.2% of dyslipidemic patients achieved LDL-C levels below 115 mg/dL [16]. Similarly, the primary care arm of EUROASPIRE V reported that only 46.9% of dyslipidemic patients reached adequate LDL-C control [17].
These results are consistent with previous studies that have highlighted the limitations of clinical judgment in risk stratification. Rossello et al. [18], in a report from the ESC Prevention of CVD Programme, emphasized the superior predictive accuracy of scoring systems compared to clinical judgment alone. Despite European guidelines recommending their use, these tools are underutilized in clinical practice. Different risk algorithms are available for various patient populations, and U-prevent.com is the only tool providing comprehensive algorithms for all categories, endorsed by the European Association of Preventive Cardiology. A recent study, by Landolfo et al.[19], have demonstrated the substantial reclassification of cardiovascular risk when employing the updated SCORE2/SCORE2-OP algorithms, particularly in populations referred for hypertension management. In their cohort of 1,539 patients, the proportion classified as low-to-moderate risk decreased from 55 to 23%, while high-risk patients increased from 20 to 38%, and very high-risk patients rose from 25 to 37%. This reclassification was accompanied by a significant reduction in the proportion of patients achieving LDL-C targets, with control rates dropping from 26 to 20% when using the Friedewald formula and to as low as 18% with the Martin and Sampson equations [19]. These findings underscore the importance of using contemporary CV risk assessment tools to refine LDL-C targets and optimize preventive strategies. Our results align with these observations, reinforcing the need for accurate CV risk stratification to guide therapeutic decisions and improve patient outcomes.
It should also be emphasized that in our study, we referred to SCORE2 and SCORE2-OP, while the risk categories referenced in the LDL-C targets of the 2019 European dyslipidemia guidelines used SCORE. However, there seems to be a slight difference in risk stratification between previous and current tools. A cross-sectional study included 85,802 patients in Hungary, and CV risk levels were determined using the SCORE and SCORE2 risk estimation methods. Using the SCORE2 method instead of SCORE, 43.91% of the population was classified at a higher risk level, significantly increasing the number of patients identified as having high or very high CV risk [9].
The slight agreement observed between perceived and calculated risk in our study emphasizes the need for enhanced integration of validated risk assessment tools in routine clinical practice. While clinical judgment remains invaluable, its complementarity with evidence-based risk scores can provide a more robust framework for managing patients at risk of cardiovascular events. Future research should focus on strategies to bridge this gap, including continued education for healthcare professionals on the utility of risk scores and the potential benefits of more nuanced risk stratification.
Traditional risk factors such as hypertension and hyperlipidemia are well recognized. However, emerging risk factors like chronic inflammation, psychosocial stress, and socioeconomic status might be underappreciated, leading to an incomplete risk assessment. In addition, current stratification systems do not capture factors such as obesity, now a recognized CV risk factor, and Lp(a) levels and familiar history of CV disease [20,21,22].
The use of tools such as SCORE2 and SCORE2-OP in clinical practice presents several challenges for clinicians. These calculators require not only a solid understanding of their methodology but also efficient integration into daily workflows. However, time constraints during consultations, a lack of familiarity with the tools, or even limited access to these resources can significantly hinder their use.
To overcome these barriers and improve adherence to CV risk calculators, several measures can be implemented: (i) continuous medical education programs should emphasize the importance of using validated risk assessment tools like SCORE2 and SCORE2-OP, training on the integration and interpretation of these tools within clinical practice is crucial; (ii) embedding risk calculators within electronic health records systems can streamline the process of risk assessment, making it more accessible and time-efficient for physicians; (iii) engaging a team of healthcare professionals, including nurses, dietitians, and pharmacists, can provide a comprehensive approach to risk assessment and management; (iv) increasing awareness of the impact of non-traditional risk factors on CV health can lead to more comprehensive risk evaluations; (v) educating patients about their own CV risk and involving them in the decision-making process can enhance adherence to preventive measures and interventions. Another promising approach involves leveraging automation and artificial intelligence (AI). By integrating AI systems into clinical workflows, these tools could automatically analyze patient data and provide accurate, personalized risk stratification. This would significantly reduce the cognitive and time burden on clinicians while ensuring consistency in risk assessment. Adapting risk calculators to better reflect local populations and contexts is another area worth exploring. While tools like SCORE2 are designed for European populations, they may not accurately capture CV risk in specific ethnic or regional groups. Tailoring these algorithms to the demographic and clinical characteristics of local populations could improve their applicability and reliability. The inclusion of emerging risk factors in future iterations of risk calculators could also make these tools more comprehensive. Factors such as chronic inflammation, psychosocial stress, and glycemic variability are increasingly recognized as important contributors to CV risk but are not currently accounted for in many tools. Finally, scientific societies could play a pivotal role by actively promoting and standardizing the use of CV risk calculators. Through awareness campaigns, development of accessible guidelines, and regular updates to tools, these organizations can help bridge the gap between evidence and practice.
By addressing these challenges through systemic changes and fostering both clinician and patient engagement, the adoption of CV risk calculators in routine practice could become more widespread, ultimately improving the precision of CV risk stratification and the effectiveness of preventive measures.
5.1 Limitations
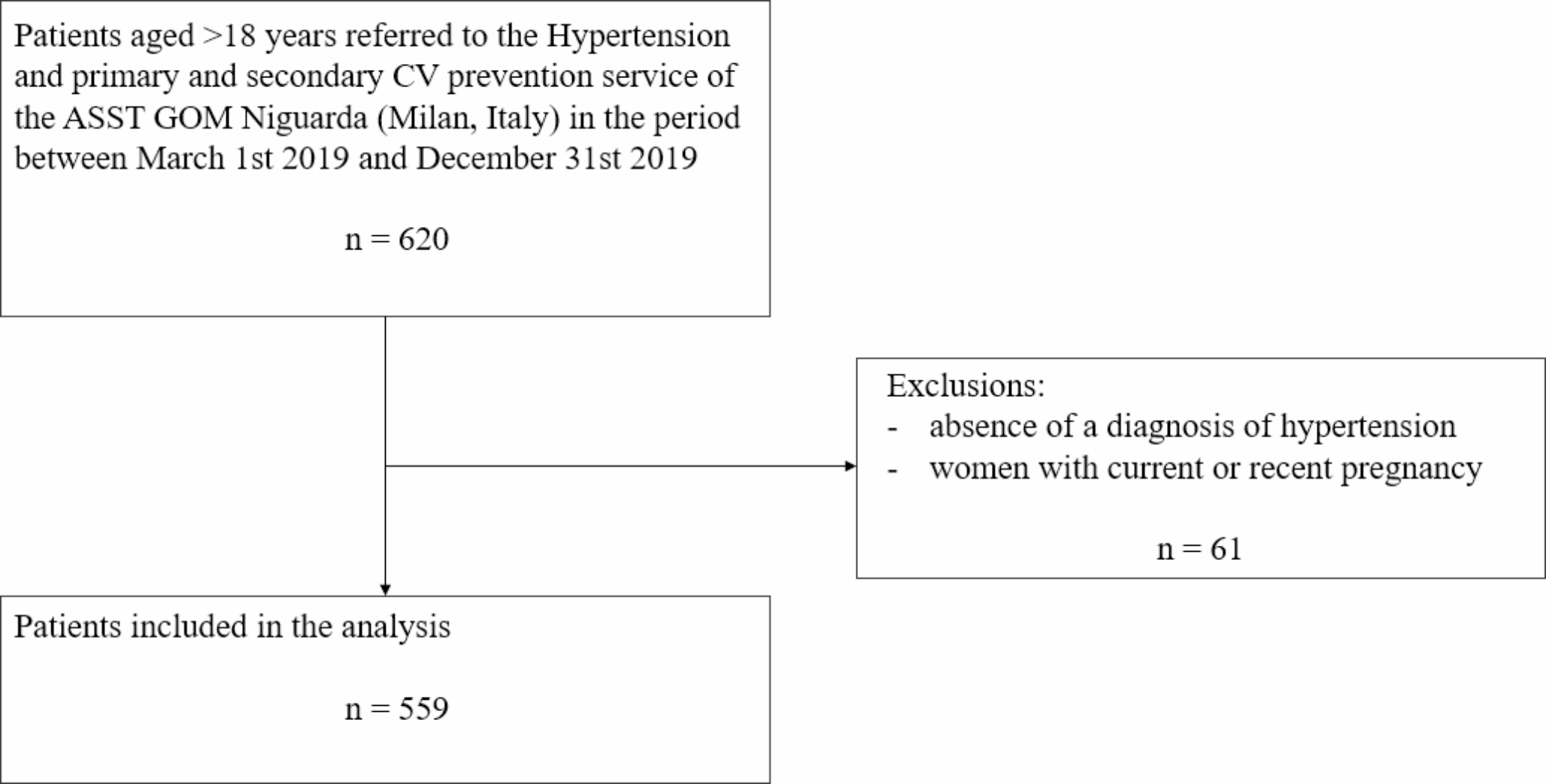
A limitation of our study is its monocentric design, which may restrict the generalizability of the findings. While this design ensured standardized data collection and assessment procedures, a multicentric approach would have provided greater robustness and external validity by incorporating diverse patient populations and clinical practices. Additionally, the cross-sectional nature of the study limits our ability to establish causal relationships between physician-perceived cardiovascular (CV) risk and clinical outcomes, such as LDL-C target achievement. Furthermore, potential unmeasured confounders, such as socioeconomic status, lifestyle factors, and adherence to prescribed therapies, may have influenced the results but were not fully accounted for in our analysis. A notable proportion of the study population (41.6%) was on antiplatelet therapy, which may reflect local prescribing practices rather than adherence to current guideline recommendations for primary prevention. This could be due to historical prescribing patterns and influenced by a reluctance to discontinue existing therapies initiated prior to referral. While these practices may introduce a potential bias, they underscore the importance of aligning treatment strategies with evidence-based guidelines. Future multicentric and prospective studies are already being planned to address these limitations, enabling the inclusion of a broader spectrum of clinical settings and patient characteristics while exploring causal relationships in greater depth.





留言 (0)