The medial canthus is located lateral to the lacrimal fossa and closely related to the lacrimal sac, which means that injury to NOE area may result in injury to the neighboring lacrimal system, or the healing process may compromise the drainage of tears [5,6,7,8,9]. Due to the close anatomical relationship between the lacrimal duct and medial canthus, the principle of staged reconstructive surgery should be to correct both the issues. To restore the naso-orbital valley and its original position, a strong enough bone fixation is needed for the medial canthus. However, to restore the lacrimal drainage system, a bony osteotomy is needed, and one needs to be careful about this. The method we introduce here is to use micro-anchors to address both issues.
With the loss of the normal traction of the medial canthus ligament, the canthus angle changes from sharp to obtuse, and with insufficient adhesion, the eyelids shorten, the medial canthus spacing increases, with the resultant disfigurement Therefore, the most important thing for the restoration of the ocular appearance is the secure, stable and accurate placement of the medial canthus ligament.
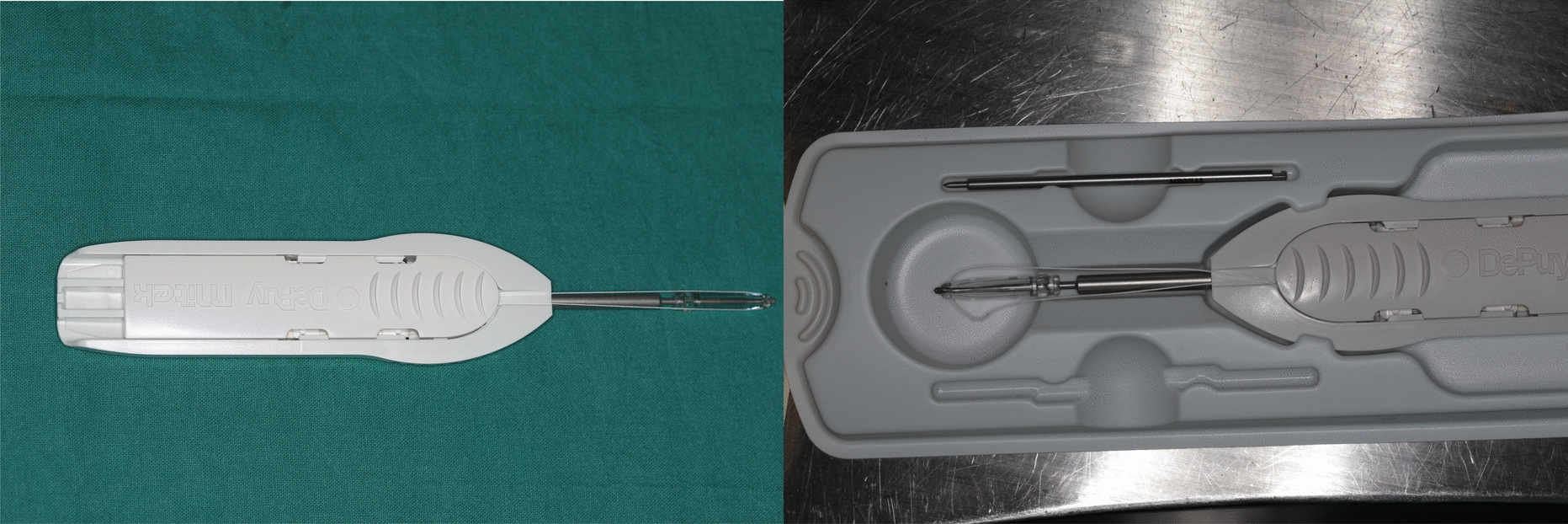
The reattachment of MCT significantly impacts facial function and appearance. Different techniques had been described, such as transnasal wiring and the Mitek Mini GII Anchor System [7]. Transnasal wiring is one of the most common techniques used in recent years. The transnasal wiring was performed after adequate exposure via the coronal incision, and surgeons needed to drill or select two (for unilateral injury) or four holes (for bilateral injury) in medial orbital wall reconstruction, which must be in the usual location of the attachment of the MCT. Kim et al. reported an oblique transnasal wiring that was performed by a Y-V epicanthoplasty incision rather than the well-known classical bicoronal approach, which could assist in minimizing unsightly scar formation [6].
To achieve good results, the fixation must be placed on a strong bone. When a lack of adequate bone limits the medial canthal ligament re-placement in the proper position, placement of a titanium plate facilitated suitable reattachment. However, this could interfere with management of nasolacrimal duct obstructions.
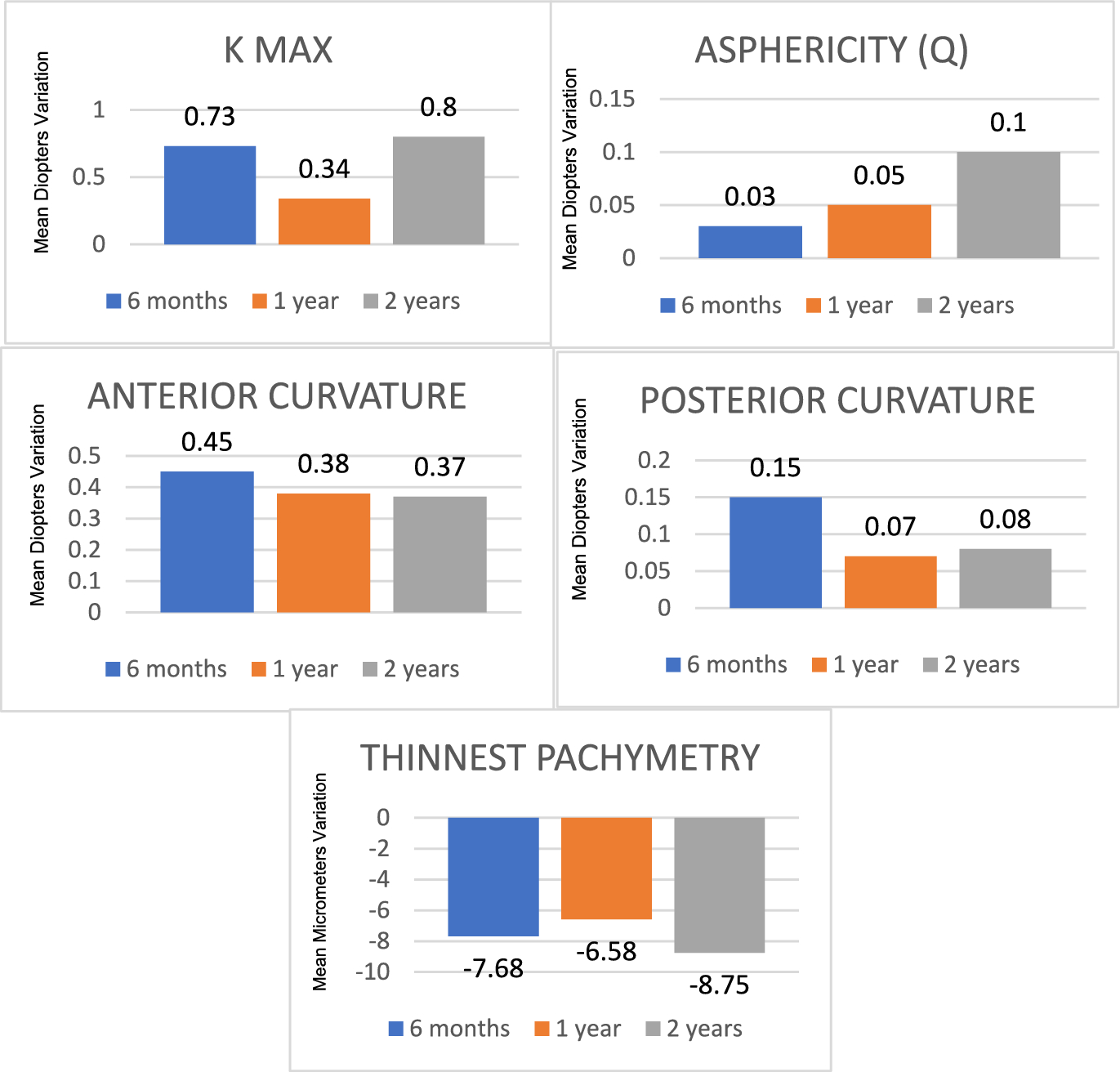
In the present series of patients, the placement of titanium screw was feasible in all cases even when there was loose bone or partial loss of bone due to the injury. The micro-anchors could provide strong attachment points for inner canthal ligament, which demonstrated long term stability and reliability in the postoperative period. Due to the small space (1.3 mm) occupied by the titanium nail and screw, performing simultaneous larger osteotomy for the DCR surgery was easier. The other advantage of these micro-anchors is their less cutting force and impact on an already traumatized bone, and the minimal space it needs for achieving good alignment of the inner canthus.
In summary, the micro-anchors and the technique used in the present study has minimal trauma, good biomechanical characteristics, good tissue compatibility, simple surgical operation, few postoperative complications, long-lasting and reliable suspension effect, and has been widely used earlier with good experience in the field of plastic surgery [10, 11]. The limitations of the present study are higher cost of the micro-anchors, smaller sample size, lack of randomization with other techniques, inclusion of unilateral cases for comparison in the same patient with the opposite side, variable ethnic and racial considerations to determine the point of MCT fixation, lack of data on accurate placement of MCT in bilateral cases, and variable follow up durations.
In conclusion, the application of micro-anchors provides the possibility of simultaneous repair of lacrimal duct obstruction and secure medial canthus fixation with excellent clinical results.









留言 (0)