
記住我

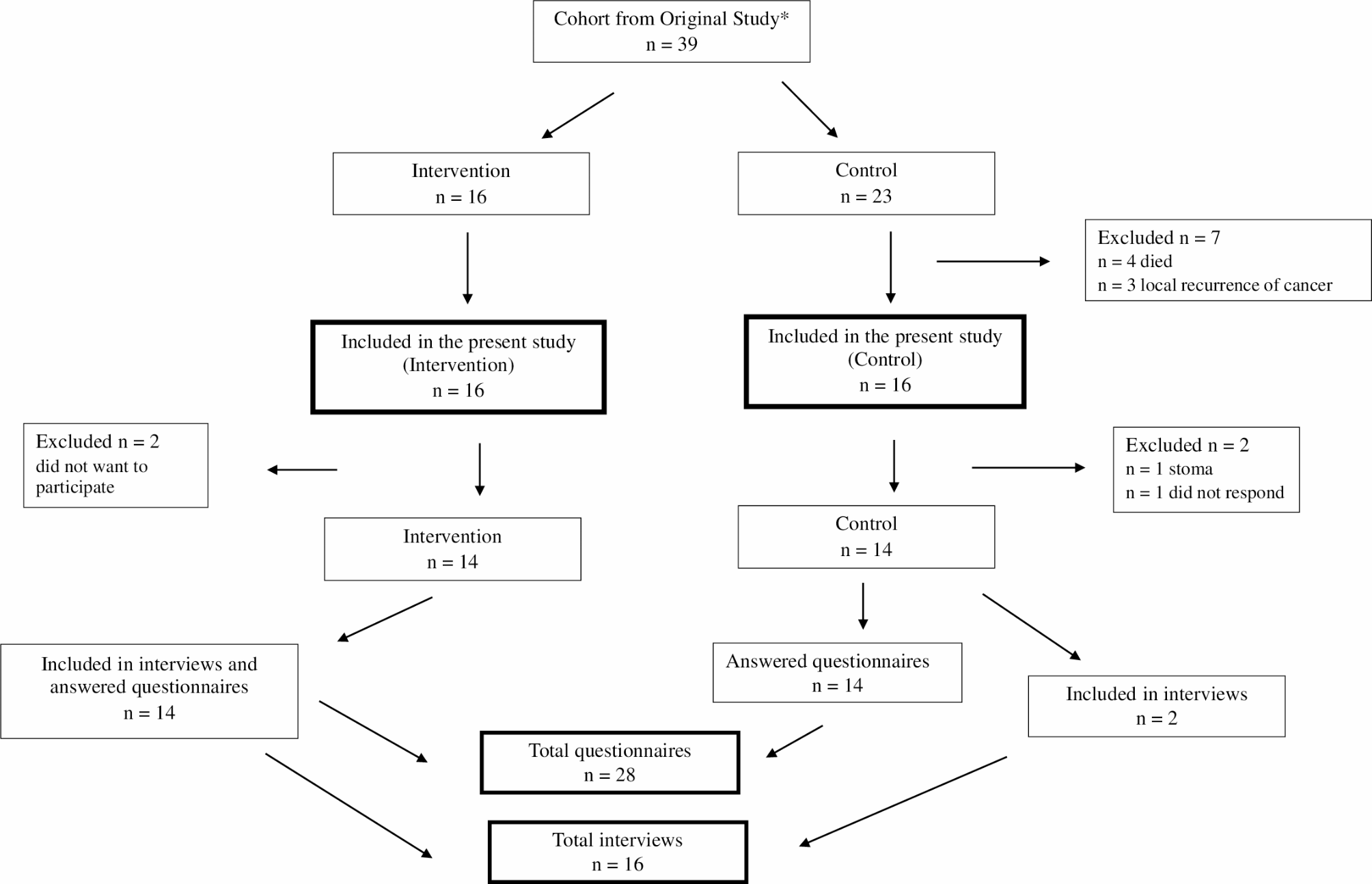





In total, 28 out of 39 patients were included in the final quantitative analysis, out of which 16 patients were included in the qualitative analysis (Fig. 1). Two patients from the control group started with TAI after the previous study ended. They remained in the control group in the quantitative analysis but were included in the qualitative analysis as they performed TAI. The mean age at primary surgery was respectively 64 years and 62 years for the TAI and control groups. There were no patients with anastomotic leakage. In both groups 5 patients received neoadjuvant radio/chemotherapy. Mean time to stoma reversal was longer for the TAI group, 212 days vs. 190 days. The mean follow-up time was 5.80 years (1.03, standard deviation [SD]) for the entire cohort, 6.04 years (0.90 SD) for the TAI group and 5.56 years (1.12 SD) for the control group (Table 2). The responses to the questionnaires from the previous study baseline (= 0 month), 6 months and 1-year were added to the results from this follow-up study.
Table 2 Patient characteristics for intervention (TAI) and control groupsFig. 1 QuestionnairesMean scores and differences between TAI and control groups in LARS Score, CCFFIS and 4-study-specific questions
QuestionnairesMean scores and differences between TAI and control groups in LARS Score, CCFFIS and 4-study-specific questionsThe mean LARS scores were similar in the TAI and control groups at study entry. The LARS score decreased significantly during the first 6 months in the TAI group (36.4 to 20.4 vs. 35.7 to 31.6). This difference − 9.4 (95% CI: -16.2 to -2.8), p = 0.0068 remained at 6-years of follow-up 21.2 vs. 30.7 in TAI and control groups respectively. CCFFIS showed no significant differences between the two groups. In the four-study specific questions, statistically significant difference in mean score, -1.6 was seen at 6 months in question 1 (“How would you describe your bowel function in general?” and in question 3 and 4 (“If you have trouble with urgency, how does this affect your daily life?” and “If you have trouble with fragmentation, how does this affect your daily life?” -2.7 vs. 2.9 respectively at 6 months in favor for the TAI group (Table 3).
Table 3 Mean scores and differences between intervention (TAI) and control groups in LARS score, CCFFIS and the 4 study-specific questionsEORCT QLQ-C30 mean scores and differences comparing TAI and control groupsAt 6-years follow-up there were no statistically significant difference in mean summary score between the groups (85.7 vs. 84.1). In contrast at 1-year follow-up the TAI group reported a statistically significant better score. The patients’ estimated global health scores were highest at 6-years follow-up, although the greatest deviation between TAI and the control groups was seen after 1-year 17.3 (95% CI: 3.8 to 30.7) p = 0.0118. Among the individual functional scales (physical and role functioning) and symptoms scales (fatigue, pain and diarrhea) significant differences (both statistical and clinical relevance) were observed at 1-year but there were no significant differences after 6-years (Table 4).
Table 4 EORTC QLQ-C30 Mean scores and differences between intervention (TAI) and control groupsComparison between TAI and control groups concerning medication related to bowel functionAt the 6-years follow-up, patients in the TAI group used less loperamide than the control group, 36% vs. 79%, respectively. The consumption of bulky agents was relatively similar, 42% for the TAI and 36% for the control group. The prevalence of any bowel regulating medication was 50% vs. 92% in the TAI and control groups (Fig. 2).
Fig. 2
Comparison between Intervention (TAI) and Control groups concerning medication related to bowel function at mean 6-years follow-up
InterviewsThere were three main categories identified in the qualitative analysis: regaining control in everyday life, need for structure and planning and becoming familiar with the procedure, all describing what role TAI had in different aspects of the patients’ lives (Table 1).
Regaining control in everyday lifeThe qualitative study revealed that TAI was an important part of the patients` everyday lives and personal well-being. The effects of TAI resulted in a more consistent and reliable bowel function. Bowel movements were experienced more consistent and emptying more complete. Patients experienced two different effects when utilizing TAI. Bowel emptying was more regular that resulted in greater predictability and fluctuation decreased which positively influenced social contexts. The frequency of bowel emptying decreased and gave a sense of increased self-control on bowel habits. TAI was also considered as a mitigant to initiate bowel emptying. A patient even expressed it as the only option, exemplified by the following citation:
“…for me it was the only way to empty the bowel.” (Patient 6).
The patients reflected that they felt less restricted in everyday life after being introduced to the TAI procedure, as they expressed improved control over their bowel function and an increased sense of self-determination over toilet visits. This resulted in the possibility to return to work and to participate in social activities as they were no longer continuously dependent on closeness to toilets. However, the patients described that their bowel dysfunction seemed to worsen when pausing the use of TAI. They perceived that TAI was necessary for a more balanced bowel function and emphasized the restored value of freedom allowing them to participate in activities. With TAI the patients experienced regained sense of self-control and no longer felt restricted in their activities. One patient even described TAI as part of life and not a treatment, exemplified by the following citation:
“… I don´t see it is a treatment, you know it is part of life…” (Patient 7).
The patients described a reduction in embarrassment and increase in confidence when discussing their bowel dysfunction and the use of TAI with their surroundings. Previously viewed as a taboo, this openness alleviated psychological distress and anxiety associated with such a sensitive topic. Regarding other symptoms such as flatus, hick-ups and an urge to open the bowel, TAI was described to have different effects and they could remain the same, disappear or improve.
Need for structure and planningThe need for structure and planning in everyday life describes how patients planned and fitted TAI in their daily routines, including the need for the correct device and place to be. The study revealed that performing TAI becomes a part of daily routine after being acquainted with the method. Patients found it to be an effective treatment and as an easy complementary solution when needed. Its straightforward nature made it easy to incorporate into their daily routine. One patient compared it to brushing their teeth, noting that it was less complicated than one might expect.
“…it goes without problem 99 out of 100 times…” (Patient 2).
Given that the TAI procedure took 45 min to 1 h, experienced by the patients, planning was essential for them. Patients described the importance of performing TAI in a calm and stress-free environment with enough time allocated to ensure that, as it is not a short toilet visit. A patient described with the following citation how one should try to eliminate stress and be able to dedicate the necessary time:
“…but you need to be prepared to allocate more time to perform in peace and quiet…” (Patient 1).
The additional planning and time management were described as providing a greater sense of control over the bowel function. With TAI, bowel emptying became more predictable and structured, in contrast to the unpredictability experienced without it. However, the intervals between each TAI procedure could lead to a feeling of being “locked in” until the next session. The patients described a need to take the possible intervals between toilet visits into consideration in daily planning. By doing so, TAI made them feel more secure in daily life even though it was not a complete solution.
Becoming familiar with the procedureThe patients found that the effectiveness of TAI relied on using the correct materials and that they had to become accustomed to the process. The TAI-kit accompanied the patients during travels, while it was extra material to bring, it was considered to be an easy accessory to carry anywhere, even to less urbanized areas. Being familiar with the instruments and the procedure made it possible to easily perform in an everyday manner as exemplified in the following citation:
“There were no issues…it felt a bit weird in the beginning, but you get used to it…” (Patient 9).
One negative aspect of TAI reported by the patients was pain or discomfort during or after the procedure. The pain could evoke anxiety and worry regarding damage to the bowel. However, these symptoms appeared to be random and could not always be linked to a specific technique or other factors even though the patients performed TAI regularly in a similar way. The pain and discomfort related to the device improved or completely disappeared after getting used to it. This is described in the following citation:
“… it was not that bad but a little discomfort in the beginning perhaps…” (Patient 5).
留言 (0)