Although numerous techniques for umbilical reconstruction have been described in the literature, this series of 50 patients is the first to present a simple and reproducible method of umbilical reconstruction during CRS where excision of the umbilicus is of oncological importance [7, 8]. Our technique is novel due to its ease, applicability and ability to be performed concurrently with CRS. Wound complications were observed in 24% of patients, the majority of whom experienced superficial surgical site infections. The complication rate is consistent with the reported 17–46% wound complication rate in the CRS literature, suggesting our technique does not carry an increased risk of wound complications [12,13,14]. No patient demographic variables were significantly associated with increased risk of wound complication.
Our data demonstrate satisfactory aesthetic results and high patient satisfaction scores while maintaining an acceptable level of wound complications. Understandably, there may be hesitancy in performing an immediate reconstructive procedure in settings with wounds are at high risk for infection, such as those with faeculant or biliary contamination [15]. However, with early recognition and appropriate antimicrobial treatment of infections, we have demonstrated no significant change in the final cosmetic result. Clinicians should also demonstrate heightened vigilance and awareness when evaluating surgical wounds, especially in cases where reconstruction has taken place.
In contrast to cosmetic surgery, open abdominal surgery for peritoneal malignancy places less (or no) emphasis on body image and cosmesis. Optimal oncological resection is the most important for outcome for surgeons, however, from a patient perspective, improved cosmesis and body image have been shown to be advantageous in improving quality of life, self-esteem and functional outcomes [16]. This is well established in breast cancer surgery, with breast reconstruction and onco-plastics becoming a sub-speciality field of its own [17]. Similarly, one of the many benefits of laparoscopic surgery is fewer scars leading to better cosmesis and improved body image [16, 18]. Unfortunately, considerations of body image are often overlooked in the context of radical cancer surgery for peritoneal malignancy: CRS significantly distorts normal surface anatomy with a midline scar, multiple drain sites and potentially a stoma. However, stomas are often reversed, and scars fade to become less prominent, leaving the lack of the umbilicus a distinct remaining anomaly. The umbilicus serves as a significant landmark and contributes to the natural appearance of the abdomen; therefore, its preservation is important to one’s body image [8].
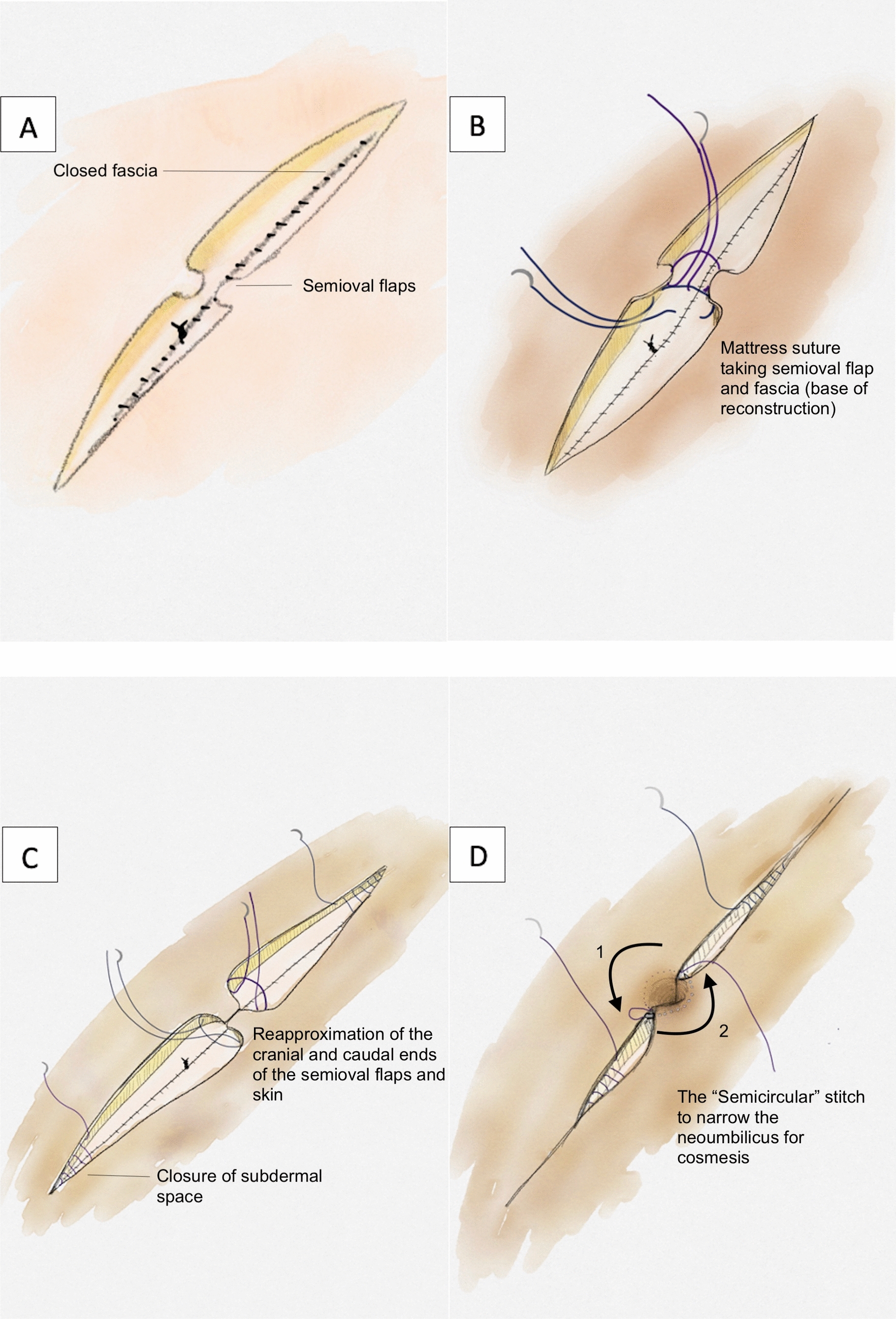
Complete reconstruction of the umbilicus or “neo-umbilicoplasty” by general surgeons differs from the usual technique of transposing the umbilicus performed after detachment during umbilical hernia operations [7]. With neo-umbilicoplasty, the precise position, symmetry and recreation of a natural-looking umbilicus are essential. This requires careful attention to detail regarding the shape, depth and proportion of the umbilicus. Joseph et al. described the “perfect umbilicus” as a vertically oriented, oval-shaped umbilicus with slight superior hooding [8]. Our described technique incorporates various elements from different techniques reported in the literature. We utilise the vertical ellipse incision and attachment of the umbilicus to the rectus as described by Bruekers et al. and Mazzocchi et al. [19, 20]. Periumbilical defatting was described by several authors and is also a fundamental component in our approach [7, 10]. Admittedly, there are a vast number of reconstructive techniques developed by plastic surgeons who perform abdominoplasties: several involves complex flaps, staged reconstruction and the use of autologous grafts to recreate the natural umbilicus shape and appearance [7]. Our technique is specifically tailored for patients undergoing maximally invasive surgery, acknowledging that achieving a perfect abdominal appearance may not be possible due to the radical nature of surgery. Thus, our aim is to offer a semblance of normalcy in an otherwise battle-scarred abdomen. One advantage of our technique is its ability to be performed concurrently with the index operation and requiring minimal additional time to perform in comparison with the entire operation. Its simplicity also allows for an easy learning curve, and the necessary concepts are readily applicable to general surgeons without requiring plastic surgical input.
This study strength includes being performed in the two highest-volume peritoneal malignancy units in Australia. We of course acknowledge several limitations including its retrospective design. The sample size is small; however, it is important to consider this in the context of the relatively rare incidence of peritoneal malignancy. This study could be strengthened by the inclusion of a direct comparison group of patients who underwent umbilical excision without subsequent reconstruction. Future prospective and randomised studies will be useful to confirm the demonstrated safety and benefits of this initial pilot study. This technique has the potential to extend further than just CRS and is transferable to other midline abdominal incisions requiring umbilical excision such as revisional ventral hernia surgery, endometriosis involving the radical excision of the umbilicus and primary tumours originating near the umbilicus.







留言 (0)