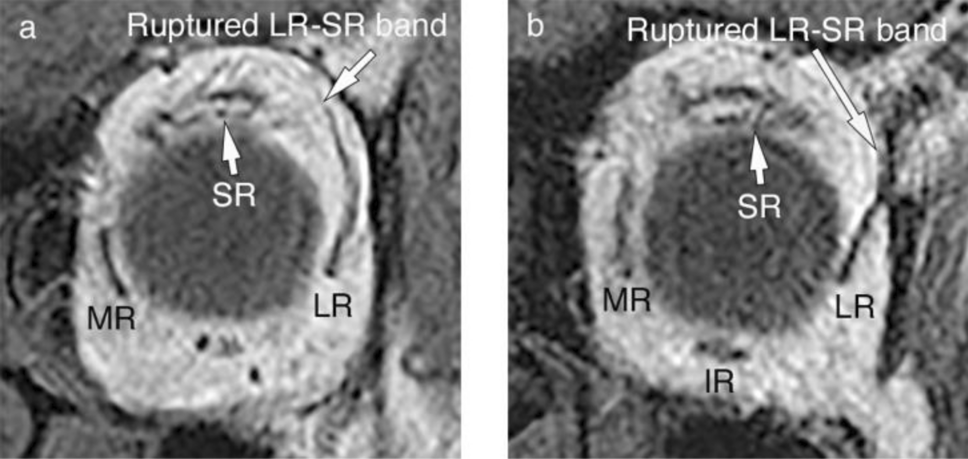
In the present study, compared to healthy young healthy participants, those with SES with full abduction and no myopia showed inferior displacement of the LR pulley and temporal displacement of the SR pulley (Table 2). In contrast, previous studies [4, 5] utilizing methods similar to ours for measuring pulley positions report inferior and temporal displacement of the LR and IR pulleys in patients with SES compared to those in young healthy individuals (average age: 28.5 years, range 21–33 years). Factors that may have contributed to the different results include the inclusion or exclusion of high myopia, variations in the participant selection methods, and potential bias introduced by the analyst when tracing the images. Chaudhuri et al. [4] report that patients with SES exhibited thinning, elongation, or frequent rupture of the LR-SR band, with ruptured LR-SR bands observed in approximately 80% of cases. In the current study, ruptured LR-SR bands were observed in all patients. In summary, given that inferior displacement of the LR pulleys and degeneration of the LR-SR band were common MRI findings in patients with SES in both the current study and previous reports, these findings warrant special attention in imaging diagnosis.
As hypothesized, the angle of the LR muscle and the inferior displacement of the IR, SR, and LR pulleys were moderately correlated, but not with the MR pulley. In contrast, the inferior displacement of the LR pulley was correlated not only with the inferior displacement of the IR and SR pulleys but also with the MR pulleys; however, it did not correlate with the horizontal displacements of the four RM pulleys.
In this study, among the patients with SES who met the criteria for the inferior displacement of the LR and degenerated LR-SR band, the correlations between the inferior displacement of the LR and the inferior displacement of the IR, MR, and SR pulleys were more pronounced in that sequence. As mentioned above, the inferior displacement of the LR pulley is one of the hallmarks imaging findings in SES; however, the inferior displacement of MR and IR pulleys varies according to the type of SES, strabismic eye, and previous reports [3,4,5, 10, 11]. In patients with SES, the correlation between the inferior displacement of the LR pulley and that of the other RM pulleys suggests that age-related connective tissue alterations could affect all four RM pulleys.
The angle of the LR muscle was correlated with the vertical displacement of the LR, IR, and SR pulleys but not with the MR pulley. Histological studies of pulleys report that the MR pulley, MR-IR band, and IR pulley have more elastin and smooth muscle cells and greater collagen content than the LR-SR band [9, 15]. Moreover, similar to the LR-SR band, the MR pulley, MR-IR band, and IR pulley also show a decrease in collagen content and thickness with age and retain more collagen content than the LR-SR band [9]. Owing to these histological characteristics, the pulley structures around the MR pulley are more easily preserved than those around the LR pulley, even in old age, suggesting that the LR and surrounding pulley structures are more vulnerable to age-related changes.
The mean (± SD) angulation of the LR with respect to the vertical is reported to be 5.7 ± 8.9° in younger healthy participants, but is significantly greater, at 17.6 ± 7.2°, in older healthy participants [4]. The LR angulation increases with aging in healthy individuals, and this increase is further pronounced in SES (22.4 ± 5.6° in DPE, 23.6 ± 13.1° in CVS) [4]. The mean LR angulation in the current study was 22°, which was approximately 4° greater than the mean LR angulation of 17.6° in older healthy participants in Chaudhuri et al.’s study [4]. In Chaudhuri et al.’s study [4], the percentage of ruptured LR-SR bands was 64% in DPE, 91% in CVS, 0% in younger controls, and 0% in older healthy participants. In this study, the percentage of ruptured LR-SR bands was 100% in SES. In the current study, the mean LR angle and percentage of LR-SR band ruptures in the patients with SES were greater than those in older healthy participants reported by Chaudhuri et al. [4], as were the patients with SES reported by Chaudhuri et al. [4].
Although healthy older adults do not show significant differences in the vertical position of the IR pulley compared to younger adults [12], the increased inferior displacement of the IR pulley in patients with SES in this study was highly correlated with the increased inferior displacement and tilt angle of the LR pulley. One reason for this could be the influence of the histological characteristics of the LR and IR pulleys. In healthy participants, the LR-SR band extends to the supraorbital side with aging [3], and the global side of the LR pulley and the orbital side of the inferior oblique (IO) pulley, where the LR-IO pulley couples, have lower collagen thickness and content [9, 16]. In patients with SES, we speculated that the same changes that cause inferior displacement of the LR owing to progressive age-related connective tissue degeneration in the LR-SR band also cause inferior displacement of the IR at the LR-IO coupling site, which has similar connective tissue characteristics as the LR-SR band and is continuous with the IR pulley (Fig. 2). In this study, the inferior displacement of the IR pulley showed the highest correlation coefficient with the inferior displacement of the LR pulley, making it the most indicative factor associated with inferior displacement of the LR pulley.
This study had a few limitations. First, this was a retrospective study with a small sample size, and both eyes of all patients were used for statistical analysis without differentiation by disease type. Additionally, it was not possible to extract the orbital MRI data of healthy older participants from medical records in the current study; therefore, a more comprehensive assessment of the conditions should be conducted with a larger sample size, by differentiating the types of diseases and adding data from healthy older participants. Second, while the positions of the RM pulleys could be compared between the patients and the control group, the tilt angles of the RMs were not available for the control group; hence, no comparison with the patient group was conducted. Therefore, the relationship between the tilt angles of the RMs and the positions of the RM pulleys requires further confirmation through comparisons in a large number of patients and healthy participants. Third, because there are no international diagnostic criteria for SES, the diagnosis in this study adhered to the diagnostic criteria outlined by Wei et al. [5]; however, cases with high myopia were excluded from the current study, and it is possible that the differences in the SES diagnostic criteria influenced the results. The criteria used for SES diagnosis differed slightly from those utilized in previous reports, such as a study that included high myopia in SES even in the absence of significant myopic degeneration [8], and a study that primarily used clinical findings to diagnose SES and excluded high myopia [1]. Therefore, caution should be exercised when comparing the results of this study with those of previous studies. Fourth, the subjects in this study included those from the period when SES was first reported [3, 4]; the diagnosis of SES was made according to the SES definition of this study, but there were some missing clinical findings and examination data in the retrospective cross-sectional case series.
In conclusion, the LR muscle angle is a valuable indicator of the inferior displacement of the LR and adjacent RM pulleys in patients with SES without high myopia. Hence, when interpreting MRI scans of patients with SES in whom uncertainty exists regarding the presence or absence of inferior LR displacement, evaluating the presence or absence of increased temporal tilt in the superior LR may prove advantageous for SES diagnosis.





留言 (0)