We conducted a study using SNDS data to analyze the before-and-after (6-month) healthcare pathway of adults who had undergone a lower extremity MRI in the second half of 2021 in France. This study updates the National Health Insurance Fund (CNAM) data from 2012 on the use of healthcare before and after lower extremity MRI. It shows that the number of MRIs has risen sharply in almost 10 years (443,242 in the first half of 2012, to 779,721 in the second half of 2021, an increase of 76%). MRI was the first-line examination for at least half of the patients (52%), even though it is not recommended.
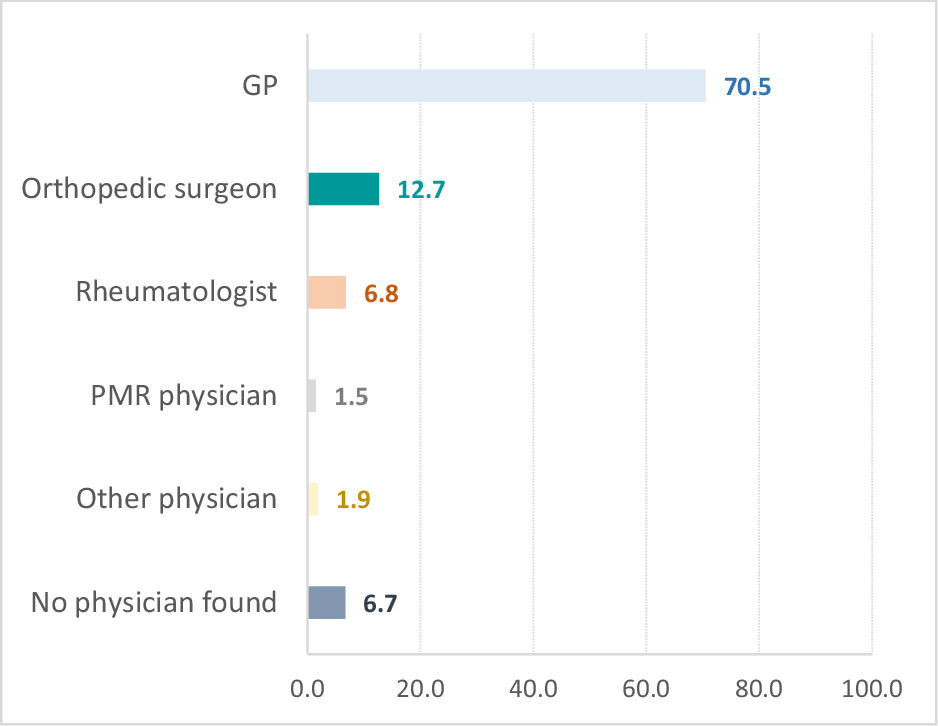
These results raise the question of the appropriateness of lower extremity MRI indications. Compared with the 2012 results observed by the CNAM, practices have not really changed. Firstly, they found that 61% of patients had not had lower extremity X-ray in the 3 months preceding the MRI. The follow-up in their study (3 months before) is shorter than ours (6 months before) and could explain why the proportion of patients without a prior X-ray observed in their study is higher than in our study. This may also be explained by the fact that they only focused on patients whose GP was the presumed requesting physician (1). However, the physician requesting the MRI is the GP for 70.5% of patients in our study, which means that the results are easily comparable. Furthermore, the CNAM observed that, among patients whose GP was the presumed requesting physician, repeated lower extremity MRI examinations were performed for 6% of patients in the 3 months preceding or following the index examination. In our study, we may also wonder whether MRI is not too frequently repeated. In fact, in the 6 months preceding or following the index MRI, 13.3% of patients had at least one other lower extremity MRI: 3.4% of patients before the index MRI and 10.6% after. Regarding the knee, the CNAM observed that less than 10% of patients underwent knee-related medical procedures within 3 months of lower extremity MRI. In our study, 20% of patients had medical procedures within 6 months of MRI. The lack of clinical data makes it difficult to evaluate the appropriateness of MRI in these patients.
Apart from the 2012 CNAM study, we have not found any other study about the relevance of lower extremity MRI or knee MRI in France. A survey carried out in 2020 by the Académie Nationale de Médecine among 260 patients seen consecutively on the same day at an osteoarticular imaging center showed that 70% of MRI requests were incomplete, with the reason for the request specified for only 14% of patients [12]. The authors underline the importance of integrating the obligation to provide sufficient clinical information into e-prescription software. Internationally, a recent systematic review of the literature concerning the appropriateness of diagnostic imaging found that for MRI of extremities, the overall appropriateness rate was 66% (n = 352/535) [13]. It is worth noting that the four underlying studies varied in sample size (55–300) and results (55–83%). One of the studies is focused on the knee; based on the availability of an electronic medical record (EMR) for every MRI performed in the Elche Health Department in Spain, the authors found that in 45% of cases (N = 135/300) the MRI prescription was inappropriate [14]. The main situations of inappropriateness included the use of MRI as the initial imaging technique. The inappropriateness of knee MRI has also been studied in other countries and has shown that practices could be improved [15,16,17]. In the USA, George et al, found that 22.8% of MRI examinations for non-traumatic knee pain realized in 2010 among Medicare and private insurance patients had been performed without prior radiography in the same calendar year [15]. In a study conducted in Atlanta (Georgia), in 2019, Gonzalez et al observed that of 196 MRIs (over an 18-month period), 57% (108 knees) had “usually appropriate” (i.e., 7-9) and 43% (8 knees) had “usually not appropriate” (i.e., 1-3) appropriateness criteria scores (p > 0.1) [16]. In Italy, in 2016, a panel of experts compared a set of guidelines with data from 400 patients who underwent previous knee MRI and found that almost 21% of prescriptions were totally inappropriate and 18.8% were uncertain [17]. The diffusion of guidelines could improve these practices. For example, a recent study by the North Bristol NHS Trust in the United Kingdom showed that the number of patients who underwent an MRI of the knee without a prior plain radiograph was 55/118 (47%) compared with 14/69 (20%) after the definition and dissemination of a referral pathway for a knee MRI [18]. In Canada, the eHealth Center of Excellence in collaboration with clinicians showed that the rate of ordering X-rays as the proper initial imaging scan for patients presenting with knee pain has steadily increased by 10% over the year for users of the eReferral platform (an integrated clinical decision support tool for diagnostic imaging requests) compared to a decrease of 7% for those using fax [19].
The main strength of our study is the use of a database covering more than 99% of the French population, which enabled us to analyze all lower extremity MRI examinations reimbursed in France. The results call into question the appropriateness of lower extremity MRI indications. They must be interpreted with caution given the SNDS limitation (mainly the lack of clinical data). It should be noted that we were unable to study the reason for requesting lower extremity MRI or to differentiate between traumatic and non-traumatic cases, as these data were not available in the SNDS. However, we excluded MRIs performed in emergency units in an attempt to focus on non-traumatic cases. In the case of repeated lower extremity MRIs, it is not possible to know whether the other lower extremity MRI is performed on the same segment of the lower extremity or even on the same side of the lower extremity as the index MRI. As a result, we may wrongly consider an examination as repeated, especially when examinations are close in time as it is unlikely that two MRIs are performed on the same part in a short period of time. Consequently, the proportion of patients who underwent a repeat MRI within a year is probably overestimated. We studied the proportion of patients who underwent a repeat MRI, considering only imaging procedures performed more than 7 days after the index MRI (Q1 of the period distribution between the index MRI and another MRI). The result is then 10.4% (versus 13.3% without a lag in the follow-up period). Nevertheless, in the absence of clinical data in the SNDS, it is difficult to differentiate appropriate practice (e.g., need for additional information due to changes in symptomatology) and irrelevant MRI (unjustified follow-up examination). Another limitation is that we chose to not include care performed on the day of the index MRI in the pre- and post-MRI follow-up, as it was not possible to know whether this care had been performed before or after the index MRI. Furthermore, the pre- and post-MRI follow-up was spread over 6 months before and after the index MRI, which may lead to an underestimation of care performed and should lead to a cautious interpretation of the results. However, this 6 months follow-up is consistent with the average time taken to access MRI in France [1], and to access surgical procedures in European countries [20].
Furthermore, this descriptive study did not have the objective to analyze the determining factors of inappropriate MRI. Analyzing whether specific age groups, genders, or other demographic factors are more likely to receive inappropriate MRIs could inform targeted educational or policy interventions. In the same way, analyzing the appropriateness rate of MRIs according to different categories of physicians could inform which physician to target. It can be noted that the physician requesting the MRI is the GP for 70.5% of the patients in our study. Although this proportion may be overestimated, we can assume that the GP is the requesting physician in at least half the cases, since in the 3 months prior to the index MRI, half the patients (52.2%) had at least one consultation with a GP, with no consultation with another medical specialty. Pending analysis of the key factors of inappropriate requests for lower extremity MRI, one of the first targets for intervention could be the GP.
Finally, it was not possible to analyze imaging practices in specific cases of knee pain. In fact, in the SNDS, only X-ray and orthopedic procedures are specific to the knee; the other imaging and outpatient procedures studied here do not allow us to distinguish the precise location of the lower extremities. We found no French data in the literature on the proportion of knee MRI among lower extremity MRI. We have performed a request on a single French hospital database and found that knee MRI represented 59% of lower extremity MRI. Nevertheless, this data does not represent the MRI practices at the national level. However, according to clinicians’ feedback on their practice, lower extremity MRI mainly concerns the knee. Subsequently, even if these results need to be tempered by the available data, they encourage us to disseminate the messages on the appropriateness of imaging in cases of knee pain published by HAS and G4 in 2022 to physicians requesting MRI (GPs in particular), but also to radiologists. We hope that the results of this study will contribute to a change in imaging practices, especially in case of knee pain. It would be interesting to evaluate these changes in a few years’ time.









留言 (0)