
記住我

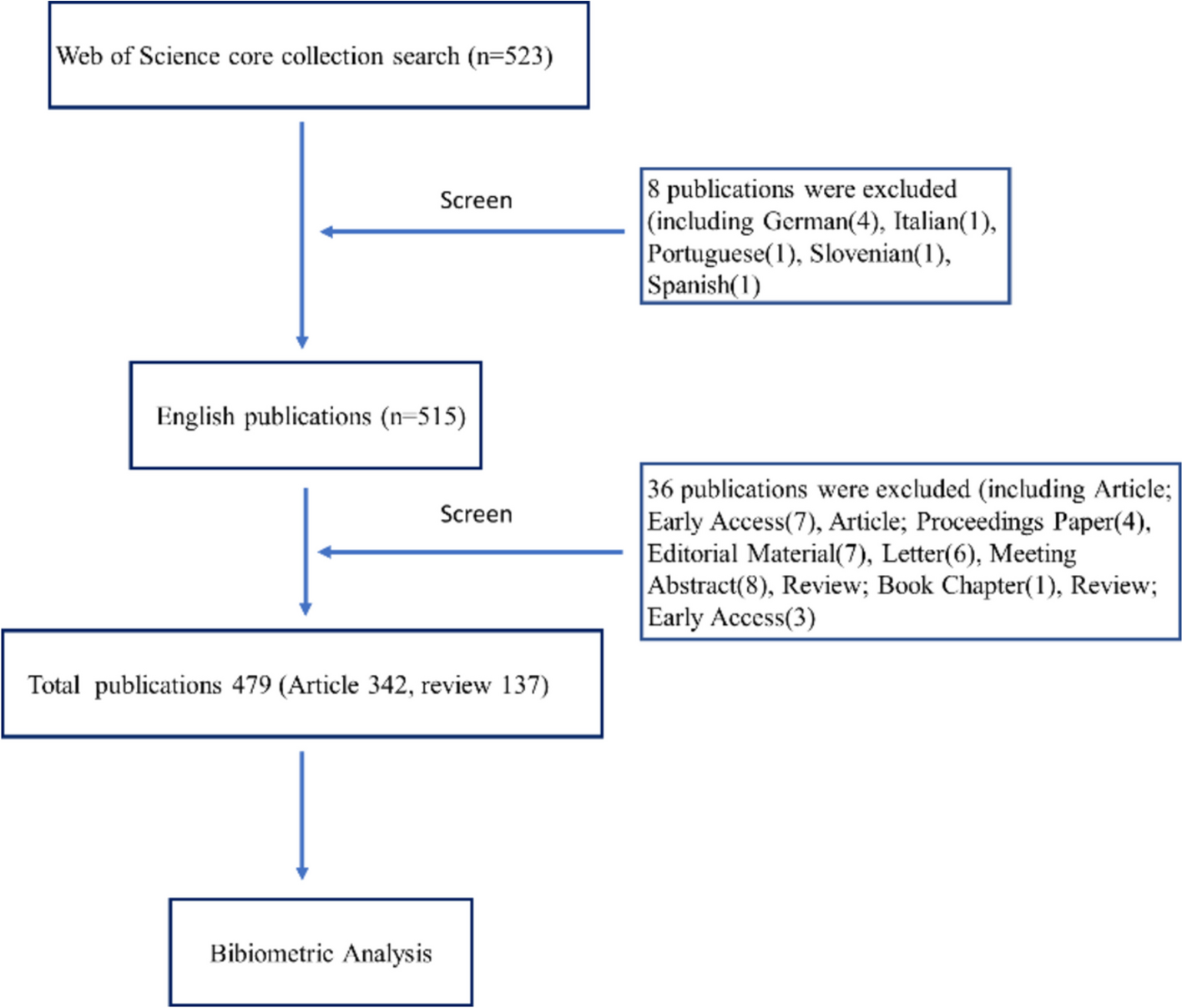





The Delphi method is a method in which investigators create a questionnaire and consult with expert group members using back-to-back communication in accordance with the specified approach. Following repeated consultation and feedback, the expert group’s viewpoints gradually become more concentrated, and the research project is ultimately evaluated based on the experts’ thorough judgments. It can accomplish the goal of brainstorming and complete development of study content through the consultation of specialists from different locations, cultural backgrounds, and expertise (Wang et al., 2018). This study uses the Delphi approach to develop a stratified nursing intervention program for POD in general wards based on literature research and group discussions, and then applies it to clinical practice to investigate the application effect, as seen in Fig. 1.
Fig. 1
Research framework diagram
Develop a stratified nursing intervention plan for PODTo obtain clinical practice guidelines and pertinent studies, a thorough literature search was done across multiple local and international databases and organizations. Appendix 1 describes the procedure of searching for literature and assessing its quality. Following the literature evaluation, group discussions were organized to plan a tiered nursing intervention program for POD in patients with Stanford type A aortic dissection. The initial draft of the strategy served as the foundation for the expert consultation questionnaire and inclusion/exclusion criteria. The nursing plan was modified and revised with the help of Delphi experts, resulting in the final document.
Quasi-experimental trial designA quasi-experimental trial was designed to evaluate the efficacy of the POD nursing care plan developed for this study. Interventions for POD were implemented using the stratified nurse intervention technique (Table 1). This quasi-experimental study was conducted in the general ward of the cardiac surgery department at a university-affiliated hospital in Wenzhou, Zhejiang Province. All patients underwent surgery by three main surgeons and were transferred to the general ward, where they were treated and cared for by professionally trained nurses.
Table 1 Nursing care plan for 2 groups patientsParticipantsDelphi method participantsFollowing a group discussion by the research group, specialists in nursing, anesthesiology, and clinical medicine were chosen for this study. Expert inclusion criteria are as follows: (1) nursing or clinical experts from a tertiary comprehensive hospital; (2) have clinical work experience in the treatment and nursing of delirium after aortic dissection, and are familiar with research in this field; (3) clinical work experience of more than 10 years, with a professional title of deputy senior or higher; (4) voluntarily and continuously participate in the entire correspondence inquiry process.
Empirical study participantsThe research, which ran from September 2022 to June 2023, included hospitalized patients with type A aortic dissections in the general ward of cardiac surgery at a tertiary hospital in Wenzhou. Patients were assigned to the control group from September to December 2022, whereas patients were admitted to the intervention group from January to June 2023. The requirements for inclusion are as follows: (1) preoperative aortic CT angiography for type A aortic dissection; (2) no history of delirium; and (3) open heart surgery with extracorporeal circulation. (4) Must be at least eighteen. Exclusion criteria as follows: (1) mortality in the hospital; (2) patient requested to discontinue treatment since the underlying sickness was progressing uncontrollably; (3) has a history of mental illness, long-term alcoholism, or drug addiction; (4) suffers from cognitive impairment, such as mental retardation or dementia; (5) due to geographical and cultural differences, unable to talk in Mandarin or dialect; (6) patients or family members requested withdrawal from the research; (7) due to therapeutic needs, patients were relocated to different departments or hospitals.
To calculate the sample size, the two-sample rate formula was used: \(n1=n2=\frac_\sqrt(1-\overline)}+_\sqrt\right]}^}^}\). According to a recent data from China, the incidence of POD is 55.68% (Zeng et al. 2021). Zhang et al. also observed a 13.5% incidence of POD in the ICU following the adoption of a delirium nursing program (Zhang et al. 2015). As a result, the incidence of POD in the control group (\(p1\)) was established at 0.5568, and in the intervention group (\(p2\)) at 0.135. Using a 1:1 sample size ratio for the intervention and control groups, and α and β values of 0.05 and 0.1, the two-sided test result produced \(n1=n2=\) 24.5889. To account for any potential sample size loss, an additional 20% was added, resulting in a minimum of 30 cases in both the control and intervention groups.
Data collectionDelphi method partTwo members of the research team contacted the experts, answered the experts’ questions, distributed and retrieved the questionnaires, and sorted out, analyzed, and extracted the consultation results. The questionnaires were sent out and withdrawn by email after the experts confirmed their consent. In order to ensure that experts completed the consultation within the specified time, the time node was reminded 1 week before the questionnaire was collected, and the interval between each round of consultation was 3 weeks. Items with mean importance assignment ≥ 4.00 and coefficient of variation < 0.25 were retained, and each item was modified, deleted, or supplemented in combination with expert opinions and suggestions. After completing the questionnaire modification, the study moved on to the following phase of expert consultation until the feedback from the experts was more consistent, at which time the consultation was ended, resulting in the final draft of the program. This study involved two rounds of expert consultations. The correspondence questionnaire contains the experts’ basic information, the importance and feasibility of each issue, and the familiarity and judgment foundation of each item.
Empirical study partThe data collection in this section was done collaboratively by the study team members and the relevant nurses. The data obtained mostly consisted of patients’ general information and intervention result. Patients’ general information was gathered through a review of electronic medical records by research team members. The nurse in charge carried out the intervention program as outlined above, recording the incidence of delirium, the time of the first occurrence, the length, and the occurrence of unplanned extubation. At 4:00 p.m. each day, study team members reviewed nursing records to collect outcome indicators and, when in question, consulted the nurse on the relevant shift.
The broad information that patients collect was developed based on a literature review and discussions within the research group (Chen et al. 2021; Feinkohl et al. 2017; Galyfos et al. 2017; Milisen et al. 2020). Including demographic and sociological data and disease status data, such as gender, age, education level, drinking, diabetes, hypertension, length of critical care unit (ICU) stays, deep hypothermic circulatory arrest time, preoperative blood lactate levels, and other postoperative problems.
The outcome measures for this study were developed based on previous research and discussions within the research group (Zhang et al. 2020). The major end measure was the rate of delirium in the general ward following surgery. Secondary outcomes were the occurrence time of delirium in the general ward, the duration of delirium, the rate of unplanned extubation, the length of stay in the general ward, and inpatients’ satisfaction scores regarding nursing care.
The Nursing Delirium Screening Scale (Nu-DESC) was used to screen for delirium in the intervention group, with five clinical symptoms assessed: disorientation, behavioral abnormalities, verbal communication abnormalities, delusions/hallucinations, and psychomotor retardation. Each item was rated on the presence and intensity of clinical symptoms, using a scale of 0 (none), 1 (mild), and 2 (moderate to severe), with a maximum score of 10. A total score of 1 or higher suggested the presence of delirium (Neufeld et al. 2013). According to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (American Psychiatric Association, 2015), patients suspected of having delirium were referred to a psychiatrist to confirm the diagnosis. Patients in the control group were observed using a delirium symptom recognition technique. Any odd behavior, such as apathy, irritation, violence, hallucinations, or disorientation, was immediately reported to the attending physician, indicating the possibility of delirium. The diagnostic criteria for delirium in the control group were the same as in the intervention group. Delirium was resolved in both the intervention and control groups when the patient’s abnormal behaviors, hallucinations/illusions, inappropriate verbal communication, and confusion stopped.
Unplanned extubation was described as the patient’s willful or unintentional removal of the tube that did not correspond to the diagnostic or treatment plan. It refers primarily to tubes other than endotracheal tubes (e.g., deep venous catheters, closed chest drains, gastric tubes). The length of stay in the general ward was determined from the day the patient was transferred from the ICU to the date of release.
Wang Lu et al. established the Inpatients’ Satisfaction with Nursing Work Scale, which was used to assess patient satisfaction with nursing care (Wang et al., 2014). This questionnaire contains 28 closed items and 1 open item, each evaluated on a scale of 1 to 5, with a minimum of 28 points and a maximum of 140 points. Higher scores imply that patients are more satisfied with their nursing care. The scale had a split-half reliability of 0.882 and Cronbach’s α reliability coefficient of 0.939. A member of the study team completed it face-to-face on the day of discharge and collected it on the spot.
Quality controlIn the research team, one deputy chief physician serves as team leader, responsible for overall work coordination and allocation, as well as providing guidance on disease treatment, medication, condition observation, rehabilitation exercises, and other related content; the head nurse serves as deputy leader, in charge of team management and daily communication with physicians. Before implementing the program, members of the study team taught the cardiac surgery nurses on the hierarchical nursing intervention for a week to ensure that they fully understood the program’s content and could use the assessment tools appropriately. Regular medical and nursing meetings were conducted to discuss the program’s implementation status. To form a Wechat working group for doctors and nurses in order to communicate patients’ conditions and nursing effects in a timely manner, at the same time, we seek to foster a positive nurse-patient connection by clearly explaining the purpose and coordination of nursing intervention to patients and their families in order to improve their knowledge and compliance.
Data analysisA database was created with Microsoft Excel, and data analysis was performed using SPSS 25.0 software. In the expert consultation section, the questionnaire’s successful recovery rate and recommendation ratio were employed to convey the positive degree of experts. Expert authority was represented using the authority coefficient (Cr), judgment basis coefficient (Ca), and familiarity coefficient (Cs). The coefficient of variation (Cv) and Kendall’s W were employed to quantify the degree of coordination between expert judgments. The mean value of importance assignment and full score rate of the items was used to illustrate the level of concentration of experts’ viewpoints. Measurement data with normal distribution were presented as mean ± SD. The comparison between groups was performed using the independent sample t test. Measurement data that did not fit the normal distribution were reported as median and quartile, and group comparisons were performed using the Mann–Whitney U test. Count data were presented as examples and percentages, and the chi-square test or Fisher’s exact test was used to compare groups. P-values < 0.05 were considered statistically significant.
Ethical considerations.
This study was approved by the First Affiliated Hospital of Wenzhou Medical University’s clinical research ethics committee (Approval number: Clinical Research Luncheon (YS2022) No. (211)) and carried out in accordance with the ethical principles of the Declaration of Helsinki and the National Research Legislation. Before the intervention, the research team members accurately and totally informed the patients or guardians about the study’s purpose, significance, substance, benefits, and dangers. The patients or guardians signed the informed consent form with their full knowledge.
Registration and inquiryThis study has been registered in the Medical Research Registration Information System of the National Health Security Information Platform, with registration number: MR-33–22–022978. The website for inquiries is www.yxyj.org.cn/www.medicalresearch.org.cn.
留言 (0)