
記住我






This study was conducted as a descriptive and cross-sectional study. The Strengthening the Reporting Observation Studies in Epidemiology (STROBE) checklist was used in reporting the study (Supplementary File).
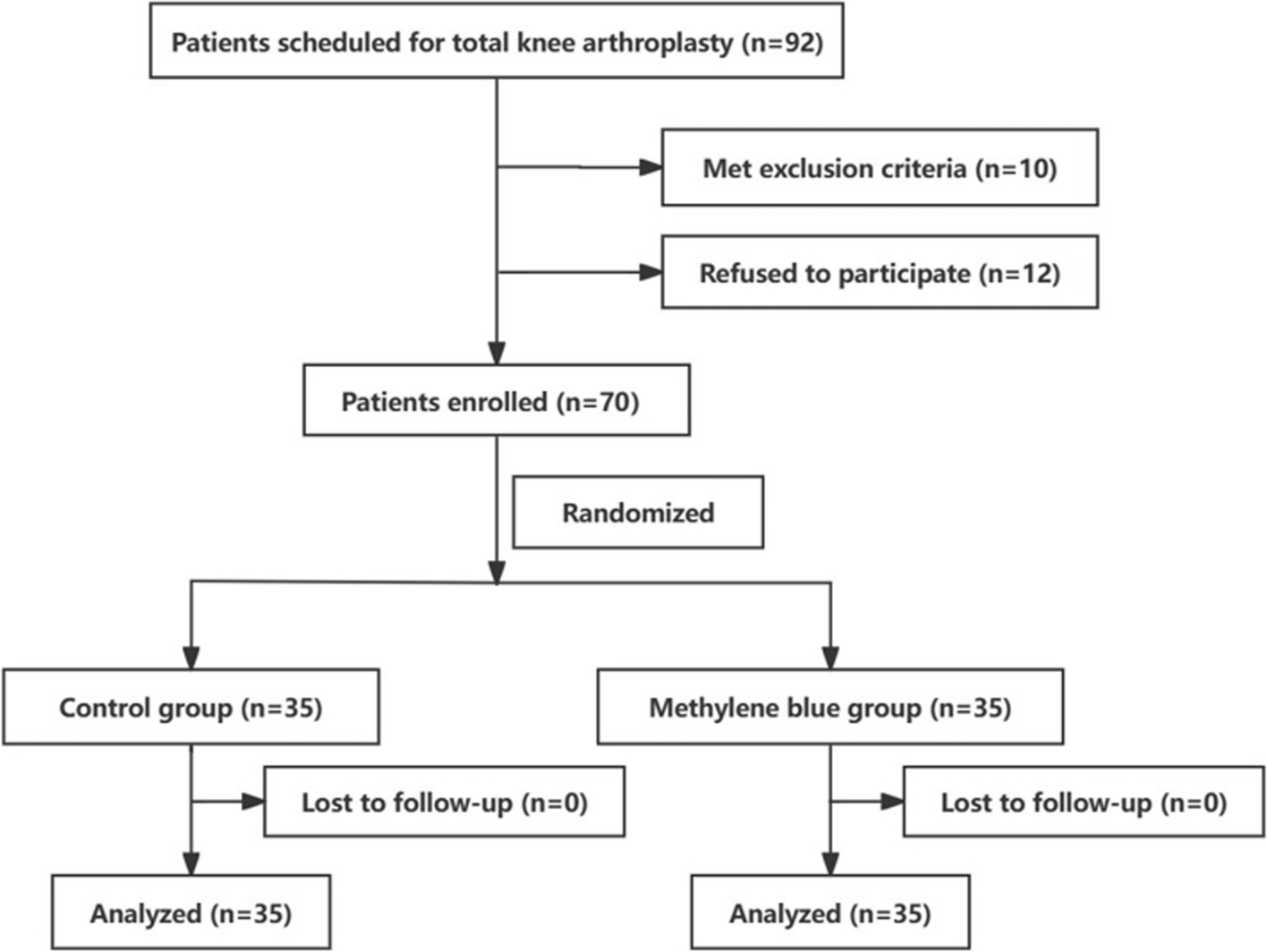
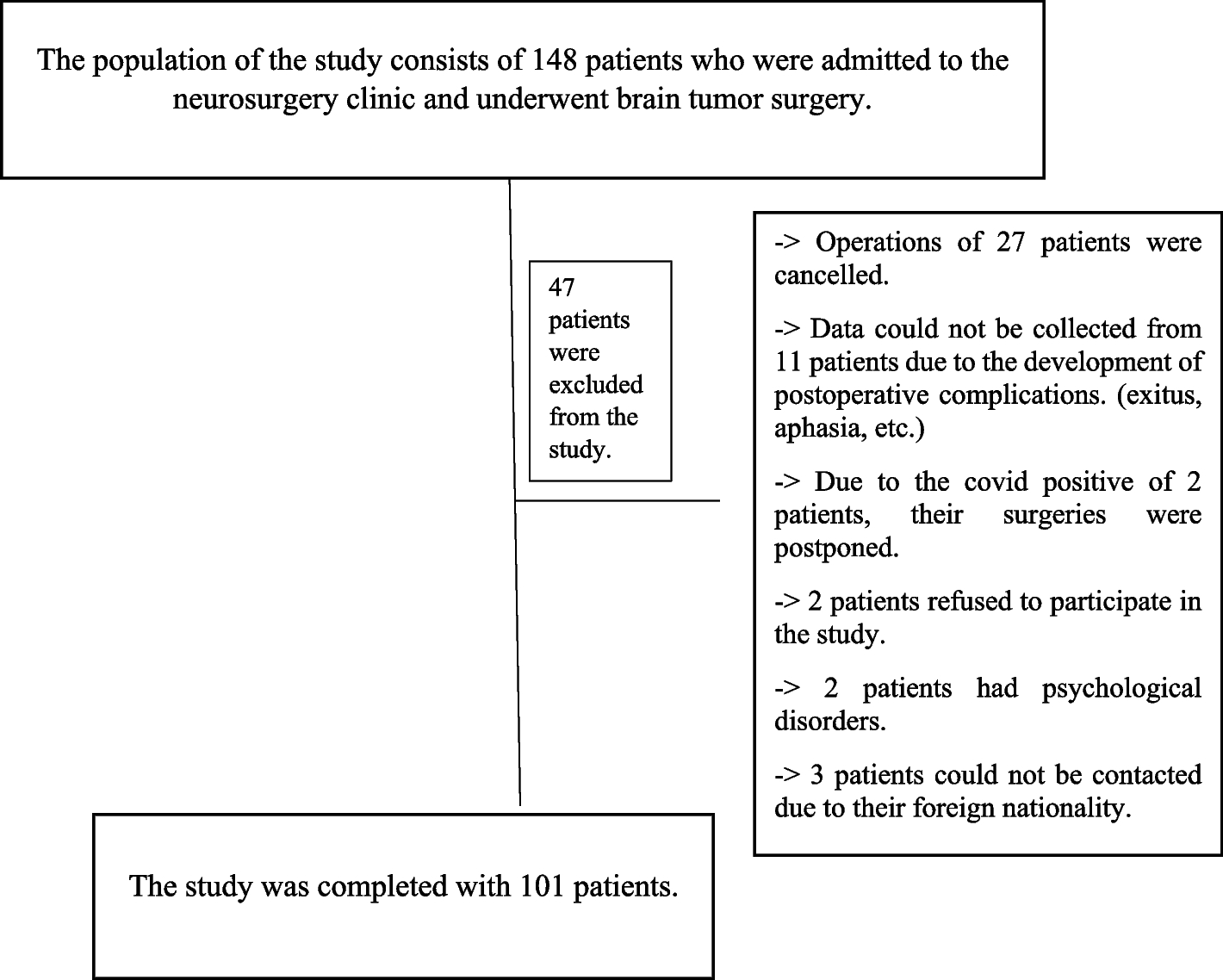
ParticipantsThe population of the study consisted of 148 patients in the neurosurgery clinic of a university hospital between October 2020 and August 2021 who underwent brain tumor surgery. This study ended with 101 patients who met the inclusion criteria and volunteered to participate in the study (Fig. 1). The sufficiency of the sample was determined according to the Post-Hoc power analyses. The effect size was obtained as 0.54 by using the correlation coefficient between the Richard Champell Sleep Scale and the Recovery Quality Questionnaire. When the Type I error was 5% and the sample size was 101, the post hoc power was 99% (Kang 2021).
Fig. 1
The universe and sample of the study
The population of the study consists of individuals who meet the inclusion criteria: (1) Those who are over 18 years old and have no communication problems; (2) preoperative and postoperative Glasgow coma score of 14 and above; (3) no psychiatric disease and no psychiatric drugs; (4) voluntarily agreeing to participate in the study; (5) patients undergoing elective surgery. (6) patients who were in the preoperative period and had spent 24 h postoperatively; (7) patients with scores I and II in the American Society of Anesthesiologists (ASA) scoring were included (Li et al 2021).
The study ending criteria are as follows; (1) patients who were included in the preoperative sampling and did not undergo surgery; (2) patients who were included in the preoperative sampling and who developed postoperative exitus; (3) when complications affecting communication such as aphasia develop after surgery.
Surgery and anesthesiaAll patients underwent surgery under general anesthesia. Fentanyl, rocuronium bromide, and propofol were used to provide anesthesia. 8 patients underwent craniotomy (tumor excision with neuronavigation and duraplasty) due to meningioma, 84 patients underwent craniotomy (tumor excision with neuronavigation and duraplasty) due to brain tumor, and 10 patients underwent transsphenoidal mass excision with neuronavigation due to pituitary adenoma.
Data collection instrumentsData were obtained using the Patient Information Form, the Surgical Fear Questionnaire, the Richard Champell Sleep Scale, the Quality of Recovery Questionnaire (QOR-40), and the Numerical Pain Scale.
Patient information formThe questionnaire form, which was created by scanning the literature (Kaya & Özlü, 2019; Bağdiğen & Özlü, 2018), consists of 16 questions including the socio-demographic characteristics of the patients (age, gender, place of residence, etc.), the duration of the surgery, the duration of the intensive care unit, the ASA score, the Glasgow Coma Scale (GCS) score, and the surgical experience.
Surgical Fear Questionnaire (SFQ)Theunissen et al. created the questionnaire in 2014 to reveal the level of surgical fear in patients undergoing elective surgery (Theunissen et al. 2014). The reliability and validity of its Turkish version were made by Bağdigen and Özlü in 2018 (Bağdigen & Özlü, 2018). The questionnaire, which is designed as an 11-point Likert scale, consists of eight items, and is scored between 0 and 10 (0 not afraid at all; 10 very afraid). The scale consists of two sub-dimensions regarding the source of fear, each consisting of four items. Items 1–4 in the questionnaire measure the fear of the short-term results of surgery (SFQ-S), while items 5–8 measure the fear of the long-term results of surgery (SFQ-L). The questionnaire total score is 0 at the lowest and 80 at the highest. A higher score indicates a higher level of fear. The Cronbach's alpha value of the adapted scale was found to be 0.93 (Bağdıgen & Özlü, 2018). In our study, Cronbach's alpha value was found to be 0.98.
Richard champell sleep scaleDeveloped by Richards et al., the scale consists of 6 items (Richards et al. 2000). Özlü and Özer performed the Turkish reliability and validity study in 2015 (Özlü & Özer 2015). In the scale, patients are asked to evaluate between 0 and 100 points for each item. The 6th item, which evaluates the noise level in the environment, is not included in the total score evaluation. The result is obtained by dividing the total point obtained from the scale by the number of questions, “0–25” points demonstrate “very bad sleep", and "76–100" points demonstrate "very good sleep". A minimum of zero and a maximum of 100 points can be collected from the scale. An increase in the score demonstrates an increase in sleep quality. The Cronbach’s alpha value of the scale is 0.91 (Özlü & Özer 2015). In our study, Cronbach's alpha value was found to be 0.93.
Quality of Recovery Questionnaire (QOR-40)The questionnaire consisting of 40 items was developed by Myles in 2000, and its validity and reliability were determined by Karaman et al. in 2014 (Myles et al. 2000; Karaman et al. 2014). The questionnaire has five sub-dimensions: comfort (12 items), emotions (9 items), physical dependence (5 items), patient support (7 items), and pain (7 items). Each item is evaluated from one to five (never, sometimes, usually, often, and always). Negative statements on the scale are scored by reversing (Myles, 2000). The score obtained from the scale varies between 40 and 200. As the score increases, the quality of recovery increases (Karaman et al. 2014). While Cronbach's alpha coefficient was 0.936 in the original study, it was 0.908 in our study..
Numerical pain scalePatients are asked to choose the number that best describes their pain intensity. While zero indicates no pain, 10 represents the worst pain imaginable (Yeşilyurt & Beneficial, 2020).
Data collectionData were obtained by the face-to-face interview method. On the morning of the surgery day, the Patient Information Form, SFQ, and Richard Champell Sleep Scale were filled in. The patient's hospitalization date, surgery date, ASA, and GCS score were recorded from the patient's file by the researcher. 24 h after the operation, the duration of the operation, the duration of the intensive care unit stay, the GCS score, and the pain score were recorded. After discharge planning, the patient was asked to fill out the quality of recovery questionnaire.
Ethical statementsEthics Committee Permission from XXX University Clinical Research Ethics Committee (Decision No: 2020/438) and institutional permission from XXX University Health Application and Research Center Directorate was obtained. Besides, verbal and written consent was obtained from the individuals participating in the research. The information was given to the patients verbally by the researcher (ÖÇ), who is also a neurosurgery nurse. The data is stored in a computer environment by the same researcher. The ethical principles specified in the Declaration of Helsinki were followed throughout the research.
Data analysisData were analyzed with SPSS 24.0 (IBM Corp., Armonk, United States). The suitability of the data to the normal dispersion was determined by the Shapiro–Wilk test, Q-Q graph, and Skewness-Kurtosis values. Student's t-test was used to compare two groups and a one-way analysis of variance was performed to compare more than two groups for normally distributed data. Mann–Whitney U test was performed to compare two groups, and Kruskal Wallis analysis was performed to compare two or more groups for data not normally distributed. In the evaluation of the relationship between the scales, Pearson correlation and Spearman correlation analysis were used. The correlation coefficient was interpreted as 0.00–0.10 insignificant correlation, 0.10–0.39 weak correlation, 0.40–0.69 moderate correlation, 0.70–0.89 strong correlation, 0.90–1.00 very strong correlation. (Schober et al 2018). Hierarchical regression analysis was done to reveal the determinants of postoperative quality of recovery. In all results, p < 0.05 was considered statistically significant. Consultation was received from the university's statistics unit.
留言 (0)