
記住我






This study was approved by the Ethics Committee of the Faculty of Medicine, Charité Berlin (EA1/044/23) and was conducted in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective nature of the study and the analysis of anonymized clinical data.
Study designThis retrospective study compared the use of the 3D 4K exoscope with the conventional microscope and assessed the learning curve using the exoscope by comparing the clinical experience with the Orbeye™ over time. This study included patients who received primary surgical treatment for oral cancer comprising microvascular reconstruction with the use of an operating microscope or exoscope during microvascular anastomosis in the Department of Oral and Maxillofacial Surgery at Charité – Universitätsmedizin Berlin at two locations, Campus Benjamin Franklin and Campus Virchow Klinikum.
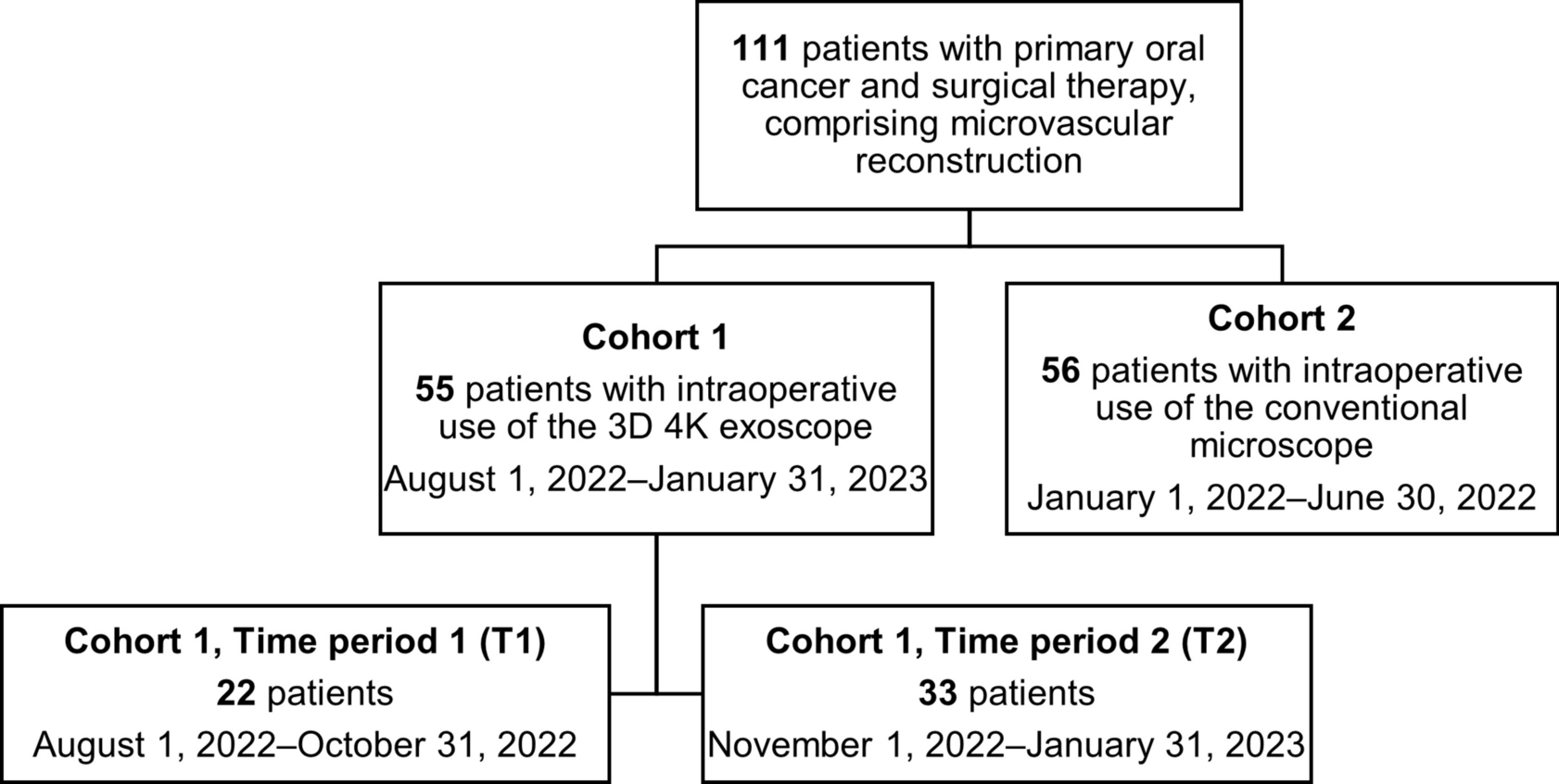
Patients were categorized into cohorts 1 and 2 according to the exoscope or microscope use (Fig. 1). Cohort 1 included patients who underwent surgery between August 1, 2022 and January 31, 2023 using the 3D 4K exoscope (Orbeye™, Olympus, Tokyo, Japan). In order to assess the learning curve using the exoscope, outcomes were compared between two time periods. The first period (T1) was from August 1, 2022 to October 31, 2022, and the second time period (T2) between November 1, 2022 and January 31, 2023. Cohort 2 served as a control group and included patients who underwent surgery between January 1, 2022 and June 30, 2022 using a conventional microscope (ZEISS S8 – OPMI Vario, Carl Zeiss AG, Oberkochen, Germany; Leica M680, Leica Mikrosysteme Vertrieb GmbH, Wetzlar, Germany). The transition period from conventional 2D microscope to exoscope use (July 1–31, 2022) was excluded.
The cohort only included patients that underwent surgical procedures for primary squamous cell carcinoma located at the oral cavity. Patients with a previous diagnosis of a head and neck cancer were excluded. Patients that had previously undergone head and neck surgery or radiotherapy were also not eligible for inclusion. The process of patient inclusion is detailed in Fig. 1, modified after Consolidated Standards of Reporting Trials (CONSORT) [10]. Data were retrospectively analyzed regarding patient demographics, type of procedure, operative duration, as well as intra- and postoperative observations and complications according to the Clavien-Dindo classification [11]. Postoperative complications grade IIIb according to the Clavien-Dindo classification within 14 days following the primary surgical procedure and postoperative complications that occurred thereafter were retrospectively analyzed. All procedures were performed by senior surgeons of the Department of Oral and Maxillofacial Surgery familiar with microvascular surgery.
Fig. 1
Flow diagram showing the patient cohorts eligible for analysis
Exoscope detailsIn contrast to the conventional microscope, the use of an exoscope eliminates the need for eyepieces and a fixed working distance. The Orbeye™ provides a 3D and 4K image, which can be visualized on one or more 55-inch or 31-inch monitors using specialized 3D glasses (Sony Corporation, Tokyo, Japan). The system allows an improved depth perception, an up to 26x magnification, and a field of view up to 171 mm. The device consists of a main unit and an extracorporeal telescope (exoscope) that contains a robotically assisted arm with a camera at its end. The exoscope can be easily steered manually in all directions. With the aid of a foot pedal, fine adjustments can be made. The near infrared image mode allows the visualization of vascular structures. Intraoperative 4K photo and video recordings can be made at any time in both 2D and 3D.
Exoscope set-up in head and neck surgeryUnlike the conventional microscope, the exoscope setup comprises multiple components, including the camera system and wired monitors. Although the multi-component system requires substantial space in the back of the operating room, the exoscope itself, featuring a small camera mounted on a slim arm, occupies little space in the operating field. This compact design allows for quick transitions between macroscopic and microscopic procedural steps.
Before the arrangement of the camera system and the monitors, it is important to consider the sterile field and the required walking paths. During reconstructive head and neck surgery, the camera arm is positioned cranially to the patient’s headrest, ensuring optimal ergonomics for the operating team (Fig. 2a, b). The sterile camera is adjusted above the surgical field to provide precise visualization for microvascular anastomoses. For instance, Figs. 2a and 3 show the favored exoscope setup for an anastomosis performed on the patient’s right-hand side, which allows the shortest distance to the monitors for optimized visualization. The set-up of the monitors and the camera system and the position of the main surgeon and scrub nurse can be mirrored, if an anastomosis is performed on the contralateral (left) side of the patient.
Fig. 2
a, b Intraoperative set-up of the Orbeye™ 4K 3D system in head and neck surgery. Two options (a) and (b) for the exoscope set-up are illustrated. The first option (a) is the favored arrangement because it allows the shortest distance between the surgeons and the monitors, but the second option (b) may be applied depending on the standardized set-up. The camera system (green) is positioned cranially to the patient’s head. The surgeons sit on opposing sides left and right lateral to the head rest (blue). The monitors (yellow) are positioned straight ahead of each surgeon, so that the surgical field on the monitor can be visualized in an upright position. This set-up serves as an example for the performance of an anastomosis on the patient’s right side so that the main surgeon (surgeon 1) is seated on the right side of the patient and has a direct view of the main monitor (monitor 1) positioned on the opposite side of the patient. The red arrows indicate the surgeons’ and the scrub nurse’s viewing directions. The foot pedal, positioned underneath the head rest, facilitates easy adjustments of the focus, magnification, illumination, and camera direction
Fig. 3
Favored positioning of the exoscope in head and neck surgery. This image, based on the schematic drawing in Fig. 2a, shows the simulated arrangement in the operating room, which facilitates the shortest distance between the surgeons and the monitors. For optimal visualization, the operating room should be darkened. In this scenario, the main surgeon is seated on the patient’s right side with a direct view of the main monitor. The scrub nurse is positioned near the main surgeon on the patient’s right side
Dual monitors facilitate visualization for surgeons positioned on either side of the patient’s head. If two monitors of different sizes are used, the larger monitor should be arranged in the viewing field of the main surgeon performing the anastomoses, considering the localizations and side of the anastomoses. Caudal positioning of the exoscope is not feasible in reconstructive head and neck surgery, especially with two team approaches. During the use of the exoscope, the operating room should be darkened, and all team members must wear 3D glasses. At the time of anastomoses, the camera itself is sterilely covered and positioned just above the surgical field by the surgeon. This also allows easy manual adjustments of the camera position, focus, and viewing field.
Statistical analysisData were collected in Microsoft Excel (Microsoft Corporation, Redmond, WA, USA), and statistical analysis was performed using IBM SPSS Statistics, Version 29.0 (IBM Deutschland GmbH, Ehningen, Germany). Continuous variables were displayed as mean or median values including standard deviations (SDs). Categorical variables were calculated as frequencies and percentages. Patients were followed-up until the last visit or date of death. The observation period ended on March 15, 2024. Overall survival (OS) was defined as the date of surgery until the last visit or date of death, whereas disease-free survival (DFS) was calculated from the date of surgery until disease progression, recurrence, last visit or the date of death. Comparisons between study groups were performed using independent t-tests for normally distributed variables. Categorical data were analyzed using chi-squared tests. P-values smaller than 0.05 were denoted as significant.
留言 (0)