
記住我






To our knowledge, this is the first publication describing the use of titanium-milled PSIs in the primary surgical treatment of unilateral, displaced subcondylar mandibular fractures. All surgeries were successful, as virtual reduction provided anatomically accurate fixation plates, and all patients had adequate postoperative occlusion with no major complications.
PSIs were planned based on regular trauma CT scans without a requirement for additional radiological examinations. Plate design took approximately 15 min of the surgeon´s time, and, due to local planning and manufacturing, the implants were manufactured and delivered within 24 h if needed. Therefore, PSI planning and manufacturing did not cause any delays in surgical treatment. The previous literature regarding surgical treatment of mandibular condylar fractures is not univocal in quality or conclusions. The most acknowledged fixation method comprises two plates, of which the posterior is aligned along the compressive strain and the anterior against the tensile strain along the mandibular notch [14, 15]. Other types of stock plates include single stock frame plates, referred to as “three-dimensional anatomical plates”, which may facilitate plate handling during surgery compared with the preeminent two-plate system. Moreover, theoretically, it may provide a more rigid fixation with reduced strain on the surrounding bone [16,17,18], but its clinical significance remains unclear [19]. Therefore, even after thorough finite element analysis (finite element method, FEM), no consensus regarding the best fixation method has been reached [20,21,22].
Postoperative complications of condylar fractures are quite rare. The most common complications include facial asymmetry, limitation or deviation during mouth opening or lateral excursion, malocclusion, facial nerve dysfunction, complications related to fixation hardware, surgical complications such as surgical site infection, salivary fistulas or sialocele formation, and hypertrophic scarring [6]. Facial nerve dysfunction is perhaps the most common complication, with a relative incidence of 0.3–28.6%, usually of a transient nature [6, 8, 9, 14, 23]. Surgical approaches entailing excessive manipulation of tissues or dissection of facial nerve branches are the most susceptible to facial nerve dysfunction [8, 9], which, as expected, is nonexistent in transoral approaches. Salivary fistulas are rare complications with a reported incidence of 1.11–2.3%. They are related to dissection of the parotid fascia during surgery and most often resolve during the first postoperative weeks [7, 14, 23]. Moreover, the rate of hardware complications, including breakage or torsion of plates and loosening of screws, lies between 1.8% and 12.2% [22,23,24]. These complications tend to occur in fracture fixations performed with a single miniplate, as opposed to other fixation methods [22, 24].
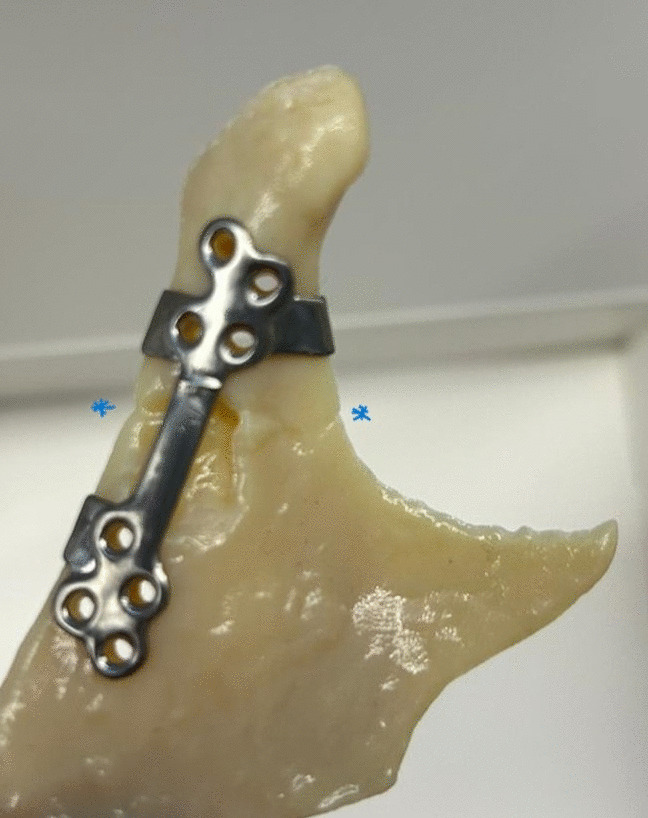
Open reduction and internal fixation of condylar fractures are technically challenging due to the requirement to manipulate the fragments in a relatively small operative field with restricted visibility, which may easily lead to complications. Thus, there is a demand for a reliable and easy-to-install osteosynthesis device. The PSIs presented here were designed to aid the anatomical placement of the implant by adding the collar-style hook around the condylar neck as seen on Fig. 5., which also helps to manipulate the condylar fragment. In addition, the indentations and tabs of the implant were intended to increase the reliability of the fracture reduction by showing the relation of the planned plate position and the fracture line. Similar implant design has previously been successfully used also for condylar head fractures [12] and zygomaticomaxillary fractures [11]. Furthermore, divergent fixation vectors were designed to increase the resistance of multiple force vectors in variable angles and minimize the risk of screws interfering with each other. A diverging screw pattern has been shown to be superior to parallel or convergent screw vectors in various clinical situations ranging from malleolar fractures [25] to tibial osteotomies [26] to radial head fractures [27] with a transfer of strain to the surrounding bone [20]. The use of PSI did not require any changes to the standard retromandibular approach. The size of the implant corresponds to the size of the standard factory-made osteosynthesis plates used in the treatment of condylar fractures. The surgical approach may even be smaller when using PSI compared to the standard two-plate fixation strategy. No other incisions were used in our study, but PSI does not preclude the use of other approaches.
Fig. 5
Postoperative dental panoramic tomography image after reduction and open fixation of the right condylar neck fracture with a patient-specific implant
To conclude, this case series demonstrated the feasibility of single-plate PSIs to treat displaced, unilateral subcondylar fractures with generally excellent results. Postoperative implant positions were accurate and satisfactory occlusion was reconstructed in all patients without major complications. Weaknesses of this study are the retrospective design, which was based on electronic patient records, and the small size of the study group, restricting conclusive statistical analyses. Further FEM and biomechanical studies may offer more profound insight into the optimal design of PSIs.
留言 (0)