This study reveals a significant reduction in CVI among JIA patients compared to healthy controls, highlighting that JIA affects the posterior segment of the eye, particularly the choroidal vasculature. These results expand the understanding of JIA’s ocular manifestations beyond anterior segment involvement, suggesting that systemic inflammation in JIA influences not only the anterior but also the posterior ocular structures [18, 19].
The lower CVI in JIA patients despite higher SFCT reflects the complexity of inflammatory processes in JIA. While SFCT captures overall choroidal thickness, which can increase due to inflammatory stromal edema, CVI specifically reflects the vascular component. Thus, although the stromal component may expand with inflammation, vascular remodeling or damage from chronic inflammation can reduce the vascular area, leading to a lower CVI. This underscores the idea that inflammatory diseases like JIA cause vascular changes that may not always correlate directly with structural thickness [12]. These choroidal vascular changes may be initiated by immune-mediated endothelial damage and microvascular compromise, contributing to CVI reduction despite preservation or increase of overall choroidal thickness [14].
A moderate negative correlation between CVI and JADAS further substantiates the influence of systemic inflammation on choroidal vascular alterations. The inverse relationship suggests that increased disease activity correlates with decreased choroidal vascularity, positioning CVI as a potential marker for evaluating inflammatory burden in JIA patients. This finding supports the notion that increased inflammatory activity results in enhanced vascular damage within the choroid. Cytokine-mediated inflammation, particularly through TNF-alpha and IL-6, contributes to endothelial dysfunction, hypoxia, and vascular remodelling, ultimately leading to diminished cardiovascular integrity as disease activity increases [20].
Although CVI showed a significant correlation with JADAS, it demonstrated weaker or non-significant correlations with other ocular parameters, such as SFCT and CMT. This finding highlights the complexity of ocular involvement in JIA, indicating that CVI may offer unique insights into vascular changes that are independent of structural modifications in the choroid. Despite the increase in SFCT, the vascular component assessed by CVI exhibited a decrease, indicating the complex influence of inflammation on ocular tissues. Balaskas et al. [21] highlighted that anterior chamber inflammation can induce subclinical macular oedema, reflecting a dynamic inflammatory cascade involving the posterior segment. This interplay between anterior and posterior segment inflammation in JIA underscores the multifaceted ocular involvement in the disease. While the correlation between CMT and systemic inflammation in our cohort was weak, these findings emphasize the complexity of retinal changes in JIA and warrant further investigation into the inflammatory mechanisms at play.
Our findings align with existing research on the ocular complications of JIA, particularly the role of posterior segment involvement [14, 18, 22]. While much of the prior literature, including studies by Heiligenhaus et al. [5] and Gueudry et al. [23], has focused on anterior uveitis as the primary manifestation of JIA-related eye disease, our study broadens this perspective by highlighting choroidal involvement. The reduction in CVI observed in this study complements earlier work that reported choroidal changes in JIA patients, such as the study by Yılmaz Tuğan et al. [18], even in cases without clinical uveitis. By quantifying choroidal vascularity, our study provides a more precise assessment of posterior segment alterations, which may be more closely tied to systemic inflammatory status than previously understood.
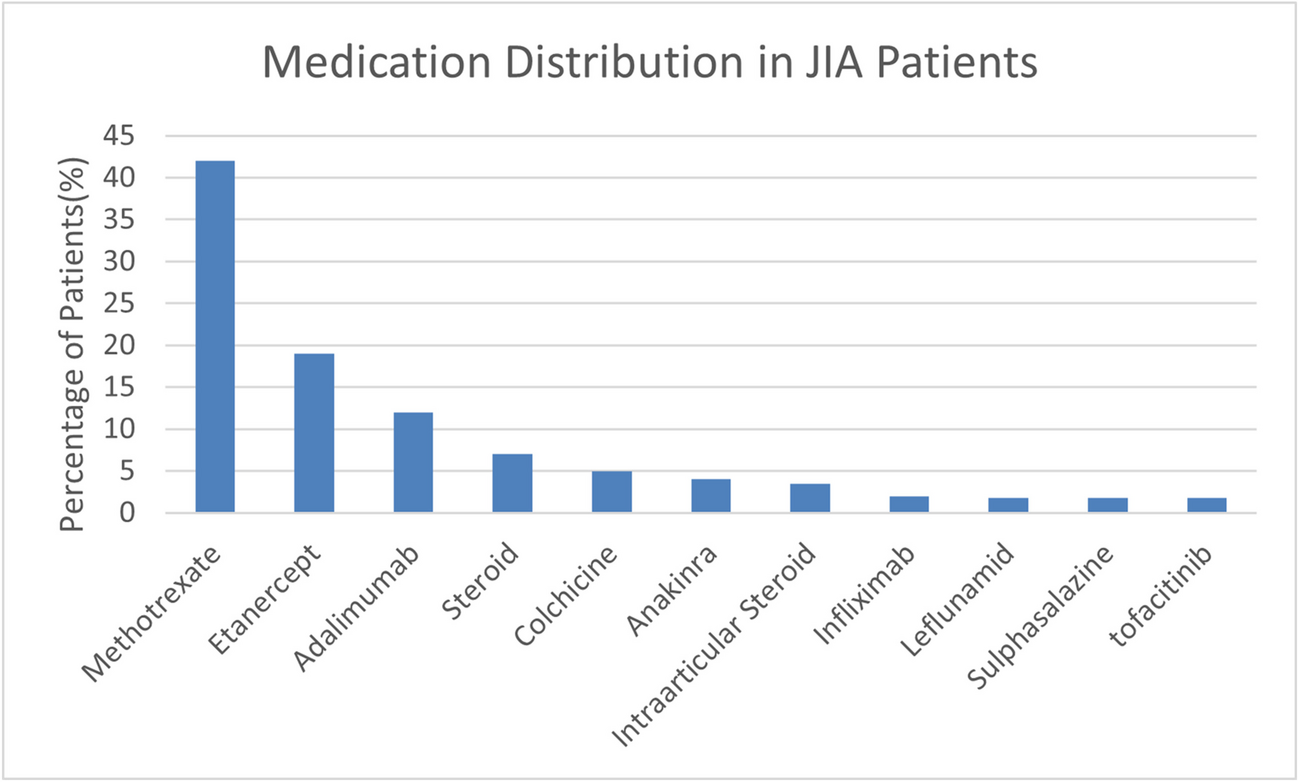
The distribution of medications among JIA patients in our study reflects current treatment strategies, with methotrexate (42%) and biologic agents such as etanercept (19%) and adalimumab (12%) being the most commonly prescribed. The systemic administration of steroids or immunosuppressants may significantly influence CVI, as these therapies modulate vascular structures and reduce inflammation. None of our patients were on topical corticosteroids, and no cases of uveitis were recorded, minimizing these factors as potential confounders. Previous studies, such as those by Kotaniemi et al. [24], have noted that biologics can reduce ocular complications in JIA, but their specific effects on the posterior segment remain underexplored. The immunomodulatory actions of these medications could influence vascular structures like the choroid and partly explain the diagnostic challenges reflected in the ROC curve analysis. Future longitudinal studies are needed to determine whether CVI changes are primarily driven by these therapies or intrinsic disease mechanisms [25,26,27].
Although the CVI demonstrated a significant difference between JIA patients and healthy controls, the ROC analysis indicated poor standalone diagnostic performance (AUC = 0.25). This suggests that while CVI alone may not be effective in distinguishing JIA from healthy individuals, its clinical utility could be enhanced when combined with other biomarkers or imaging parameters. Low specificity at the optimal threshold would suggest that CVI is more sensitive to early changes in the choroid and could therefore give false positives if used in isolation.
The association of CVI with JADAS nonetheless supports the use of CVI as a "monitoring tool" rather than a sole diagnostic marker. Specifically, the incorporation of CVI into routine ophthalmic assessments may provide better monitoring of disease progression or therapeutic response in patients with JIA, where systemic inflammatory markers do not always incompletely represent localized ocular inflammation. Unlike more conventional inflammatory markers, CVI may provide unique insights into how systemic inflammation affects the eye over time [28] With the fact that clinicians measure CVI regularly, early detection of choroidal involvement may be possible, thereby interceding before overt clinical symptoms of uveitis.
If standard systemic markers are not sensitive or adequate to capture subclinical ocular changes, CVI might fill this need as a non-invasive means of quantification in ocular health. This may be especially pertinent for patients undergoing biologic or other immunomodulatory treatments, as the supplementary data from CVI could signify the efficacy of these therapies and guide the modification of treatment protocols [28, 29].
This study has several potential limitations, including a small sample size, a cross-sectional design, and insufficient control for confounding factors such as medication usage and disease duration. Larger multicentre studies are needed to confirm these findings and further investigate possible differences among the various JIA subtypes. Longitudinal studies that follow the course of CVI over time and with treatment are needed; this would further elucidate how choroidal vascularity changes with disease activity.






留言 (0)