Using real-world data, we found that physicians administered adjuvant TCH, tH, or AC-tH or neoadjuvant TCHP and adjuvant trastuzumab to 64.3% of the 6474 patients with HER2-positive BC covered by health insurance plans in our study. The 5-year OS rate was 96% for these patients. These regimen patterns reflect the evolving landscape of HER2-positive BC treatment according to U.S. FDA approval of new drugs and the National Comprehensive Cancer Network treatment guidelines.
Our findings regarding treatment regimen patterns were similar to those in other studies. In an older study before the incorporation of pertuzumab to the treatment of patients with early-stage BC (2008–2012), Giordano et al. [14], observed that TCH and AC-tH were the two regimens given most frequently to patients receiving trastuzumab (~ 57% and ~ 17%, respectively). We report similar findings in the same time period, with TCH and AC-tH being the most common regimens in our study (~ 47% and ~ 13%, respectively). Bari et al. [15] reported that the most commonly used adjuvant regimen among patients with 70 years of age or older was tH.
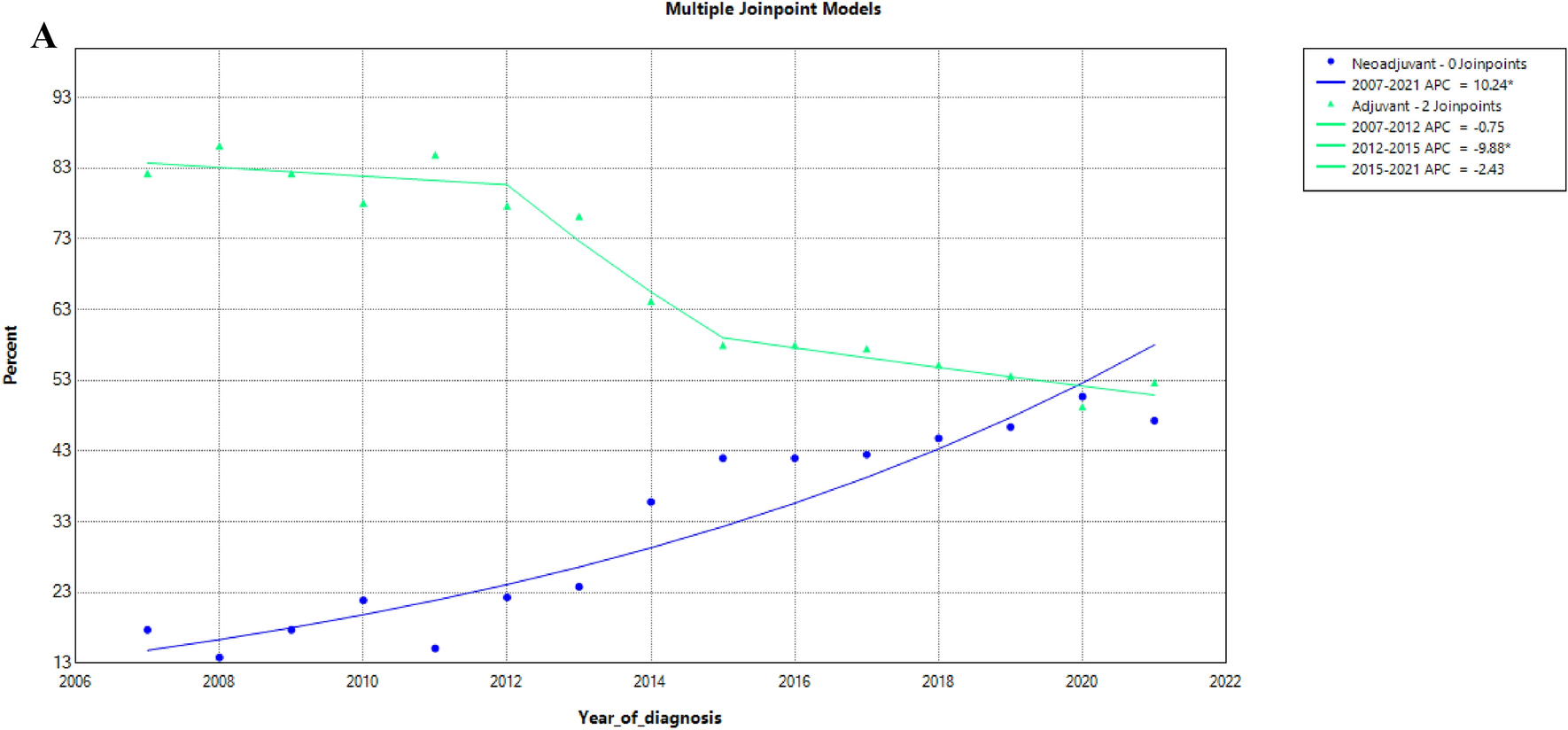
Our findings regarding regimen patterns and trends reflect the evolving NCCN treatment guidelines for HER2-positive BC and demonstrate some differences between real-world patterns and the NCCN guidelines. Since pertuzumab was approved by the FDA for use in the neoadjuvant setting in 2013, the use of neoadjuvant TCHP followed by Trastuzumab and pertuzumab increased, whereas that of adjuvant TCH decreased (Fig. 1C). Similarly, the use of adjuvant tH notably increased, reflecting the changes in practice associated with the results of the ATP trial, showing that among patients with node-negative disease adjuvant tH was associated with a 7-year disease-free survival of 93%[16]. These pattern changes correspond to changes in the NCCN guidelines for HER2-positive BC in 2014 and 2018, respectively. Something worthy to mention is that although the NCCN listed FEC in combination with trastuzumab as a potential regimen in 2014, the clinical uptake of FEC has remained very low (less than 30 patients in our cohort since 2014). This may be due to the no survival benefit of FEC in the FinHer trial or more likely to the concern for increased cardiotoxicity associated with the use of anthracyclines [17, 18].
We observed notable changes in treatment patterns with an important increase in the use of neoadjuvant therapy after 2007. Advantages of using this approach include downstaging and the possibility of performing less extensive surgery with improved surgical outcomes. In addition to providing an in vivo assessment, given the important opportunity for evaluation of whether patients have residual invasive disease in the breast or axillary nodes or if they achieve a pCR [19]. Today, patients with residual disease can be candidates for more effective treatment with adjuvant T-DM1 based on the improved outcomes seen in the Katherine trial [9]. Neoadjuvant therapy is recommended for patients with stage II or III HER2-positive BC. For those with stage I disease or small, node-negative tumors, surgery is usually the initial treatment, and the tH regimen is commonly used. Unfortunately, our study could not explore the use of specific regimens according to lymph node involvement, as claims data lacked this information.
Of relevance, the patients in our cohort had high survival probability, with a 5-year OS probability higher than 90% for the 15 trastuzumab-containing regimens. Suggesting that regardless of the regimen used and patient characteristics, current treatment is associated with excellent prognosis. Patients who received neoadjuvant regimens recommended by NCCN had a 5-year survival probability of at least 95%. Among the patients who received adjuvant regimens, only those who received TCH; tH; or docetaxel and trastuzumab had a 5-year survival rate of at least 95%. We report a slightly better survival among patients treated with neoadjuvant compared to adjuvant therapy. This result needs to be interpreted with caution since there are important tumor and patient characteristics that we cannot account for, in addition of indication bias. Patients treated with neoadjuvant chemotherapy had likely more extensive disease and because of that reason, given regimens considered to be more aggressive or effective by their physicians. It must be noted that about 90% of patients in our study who received neoadjuvant therapy after 2013 received pertuzumab-containing neoadjuvant regimens. Gianni et al. showed that pertuzumab used in neoadjuvant settings led to a higher pCR rate than those not receiving pertuzumab [6]. In addition, it is well known that pCR is associated with improved survival [20] providing in vivo assessment of response which can guide physicians to switch adjuvant therapy to T-DM1 if there is residual disease after neoadjuvant therapy. Therefore, patients treated with neoadjuvant therapy were diagnosed in more recent years than patients who used adjuvant therapy. Patients who used adjuvant therapy in 2013 or prior had longer follow-up times which was associated with a higher risk of death than neoadjuvant patients who had a shorter follow-up time.
Besides the survival differences between neoadjuvant and adjuvant therapy, our study demonstrated that patients with HER2-positive, hormone receptor-positive BC had a lower risk of death than patients with hormone receptor-negative BC, which confirmed the results of other studies [21, 22]. Some regimens in our study showed inferior survival compared with results from clinical trial studies. For example, in patients given adjuvant pertuzumab and trastuzumab combined with chemotherapy in the APHINITY trial, the 6-year OS rate was 95% [23], which was higher than our 5-year survival rate of 93% (with 95% CI 87–98%) for the adjuvant TCHP group. It is well known that the results of clinical trials are not always exactly mirrored in the general population, it should be noted that in the APHINITY trial, 13% of the patients were at least 65 years old, whereas, in our adjuvant TCHP regimen group, 32% of the patients were at least 65 years old. In addition, it is well known that clinical trial participants tend to have fewer comorbidities [24] and are more compliant. In particular, the patients treated in the APHINITY trial were likely associated with a lower risk of death compared to the real-world population.
Our study had several strengths and limitations. A strength is that we evaluated the regimens based on health insurance data with a large cohort of 6474 patients diagnosed with HER2-positive BC for 15 years. We depicted the regimen patterns and trends corresponding to new drugs made available for the treatment of HER2-positive BC and the evolution of NCCN guidelines. We were able to identify the study patients’ regimens using health insurance claims data, however, we used BC surgery and trastuzumab-based chemotherapy administration as a surrogate to define HER2-positive early-stage BC using claims data. We cannot exclude that some patients with advanced BC were included in the cohort, since we do not have stage information. However, this number was likely small. In addition, without lymph node status in the claims data, we were not able to determine the regimen patterns or outcomes for patients with node-negative disease. Likewise, we lack data on patients who had medical conditions or factors that prevented them from receiving anti-HER2 treatment, or who were not considered candidates for systemic therapy. Also, we did not evaluate the drug use sequence, dosage, or treatment cycle length for the regimens in this study. This may have led to an underestimation of the regimens’ treatment effect, as concurrent and sequential drug use have different treatment effects and toxicity. Future studies of the development of algorithms to identify real-world dosages, drug use sequences, and treatment cycles for HER2-positive BC treatment regimens are needed to understand the association of regimens with toxicity and also with the risk of recurrence and survival. Finally, we used CDM data in this study, which may not be generalized to other patients with different types of health insurance coverage or who have Medicaid or Medicare coverage.
In future studies, we will evaluate the HER2-positive BC treatment patterns and trends in Medicare beneficiaries to gain deeper insights into the association between regimens and survival.



留言 (0)