Here, we present the baseline data of retina macular microperimetry, OCT and OCTA in idiopathic ERM, and the relationships between macular focal sensitivity with retinal microstructure and microvascular parameters in ERM patients related to EIFL. ERM patients with EIFL exhibited significantly reduced macular sensitivity in MSmacular compared to those without EIFL, as well as in MSfoveal and MSparafoveal. Additionally, ERM patients with EIFL demonstrated significantly increased VDfoveal and PDfoveal compared to patients without EIFL; however, the VDparafoveal was significantly decreased. LASSO and Quantile regression analysis revealed that increased VDparafoveal positively influenced the light sensitivity of MSfovea, whereas the presence of EIFL negatively impacted the light sensitivity of MSfovea in patients with ERM.
Considering the possibility of participants’ fatigue, minimal learning effect, and similar repeatability [8, 16] of microperimetry results during the test, we adopted a short training and practice model to conduct microperimetry. Thus, our results suggest that microperimetry not only showed results consistent with the trends of visual acuity but also demonstrated subregional effects of the ERM on the local macular area. Feng and colleagues [10] recently analyzed MP-1 microperimetry variation in a cohort of 30 patients with ERM who underwent pars plana vitrectomy surgery. Using a grid with a diameter of 10°, they noted a rising trend in macular sensitivity after ERM peeling surgery, suggesting that ERM in the macula can decrease macular sensitivity.
Our results indicated that macular sensitivity was significantly lower in ERM patients with EIFL than in those without EIFL preoperatively. The topographic assessment provided by microperimetry testing in this study revealed that stabilized and undisturbed anatomical structure of the inner retinal layer play an important role in maintaining the stability of macular sensitivity, not only in the foveal area, but also in the parafoveal area.
The unique anatomical configuration of the fovea and parafovea results from the displacement of centrally distributed photoreceptors combined with the ‘Müller cell cone’ and the ‘z-shaped’ pattern of parafoveal Müller cells [17, 18]. The presence of ERM may exert both centrifugal and contractile force on the macular surface, leading to deformation of the inner retinal layer. Additionally, the occurrence of EIFL may disrupt the balance maintained by Müller cells, resulting in the disorganization of the photoreceptor layer. Previous studies have identified that factors such as disruption of EZ integrity [3], central macular thickness [2], and alterations in photoreceptor outer segment length [19] correlated with preoperative and postoperative visual acuity. In this study, we identified disruption of EZ integrity and increased CFT as risk factors that correlate with microperimetry, which is consistent with the findings related to visual acuity. The observed increased CFT and disruption of EZ integrity were statistically associated with a decline in macular sensitivity. The decline may not only be attributed to the disruption of the balance of vertical and horizontal forces by Müller cells, but also to the exacerbation of Müller cells activation.
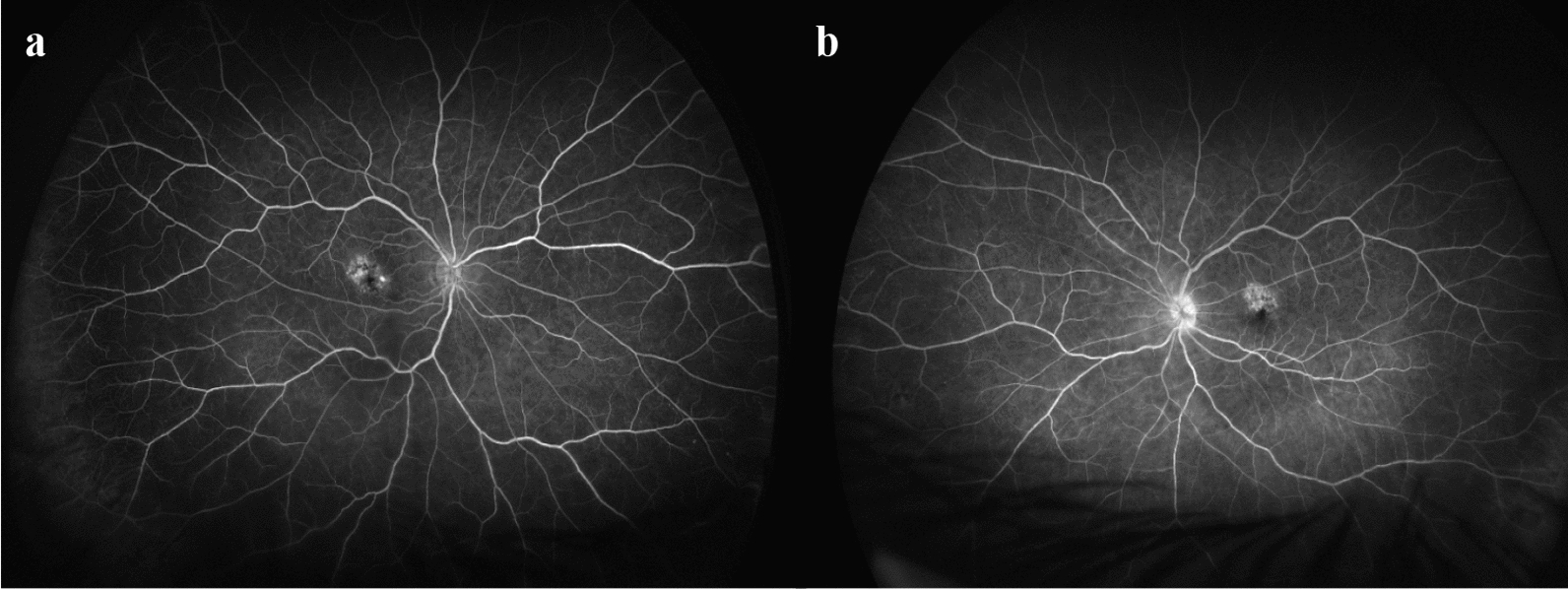
The ERM not only affects inner retinal layer microanatomy, but also impacts the inner retinal layer microvasculature. Here, the OCTA analysis in eyes with ERM showed increased VD and PD in the foveal area along with a statistical decline in microperimetry parameters, demonstrated that retinal microvasculature density in the foveal area is a determining factor for light sensitivity. Physiologically, the diaphaneity of fovea tissue in the foveal pit, which overlies the photoreceptors, assures specialization for high visual acuity [18]. The presence of ERM significantly altered the FAZ, varying from a capillary-free zone to an area of near-complete obliteration of the FAZ in ERM eyes with EIFL. The increased microvasculature in the foveal area may cause light scattering and absorption by blood vessels, thereby blocking incoming light and resulting in a reduction in visual sensitivity [20]. This hypothesis was also validated by studies in age-related macular degeneration and Macular Telangiectasia [21, 22].
In this study, decreases in ‘total vessel length’, ‘average vessel length’, ‘total number of junctions’, and ‘junctions density’ were found in ERM eyes with EIFL. These parameters represent the division of the lengths and branch junctions of all vessels. Thus, the decrease in vessel length and branch junctions indicates that the vessels become more linear in shape, and the traction force by ERM made the vessels less tortuous. In tandem, Miyazawa et al. [23] quantified the macular vessel tortuosity with ERM following surgery and indicated that it was associated with visual outcomes after surgery. Moreover, Feng et al. [10] demonstrated that the release of ERM traction with surgery could improve postoperative visual results, indicating that increasing the parafoveal VD through the release of these taut vessels would be beneficial for light sensitivity.
Our study illustrated that VDparafoveal depicts a positive effect on MSfoveal, suggesting that a higher concentration of microvasculature in the parafoveal area correlates with increased foveal sensitivity. From an anatomical point of view, the blood vessel parameter analysis using Angiotool revealed that vessel length and junction density decreased under the influence of ERM with EIFL. From the perspective of retinal metabolism, under physiological conditions, Müller cells in the central fovea tissue not only provide structural support to the fovea but also facilitate functional and metabolic interactions with photoreceptors [18]. However, under pathologic mechanical stress, such as that induced by the presence of ERM, retinal injury can activate Müller cells through various mechanisms and trigger reactive gliosis [24]. Therefore, we hypothesize that the observed positive correlation between VDparafoveal and MSfoveal may not only be a phenomenon induced by ERM, but also could be a result of increased metabolic demands following morphological alterations in the fovea. The underlying pathophysiological mechanism contributing to VDparafoveal and its positive effect on MSfoveal remain speculative; however, they may provide new insights into potential therapeutic strategies for ERM. This factor could influence surgical decision-making in ERM patients with EIFL.
The current study has several limitations. First, it was a baseline structure and function analysis in which no adjustments were made for multiple comparisons and no long-term observation took place. Factors like lifestyle (smoking, alcohol consumption), nutritional status, and environmental exposure could have been considered. Second, the accuracy of microperimetry depends on the participants’ mental state and cooperation, which could vary between patients or even within a patient over time. To avoid this bias, all patients completed a uniform two-minute training session prior to beginning the test, and we excluded the values obtained during the training. Third, metamorphopsia is one of the major symptoms in ERM patients, and it is better to quantitatively measure it using M-CHARTS [25] instead of the Amsler Grid Test, as was done in the present study.









留言 (0)