
記住我
Prior to the study, ethical approval was obtained from the Inonu University Health Sciences Non-Interventional Clinical Research Ethics Committee (2022/557). The study was designed retrospectively, utilizing serum samples collected during the pandemic period. Analyses were conducted at the Immunoassay Development Laboratory of the Inonu University Medical Faculty Physiology Department.
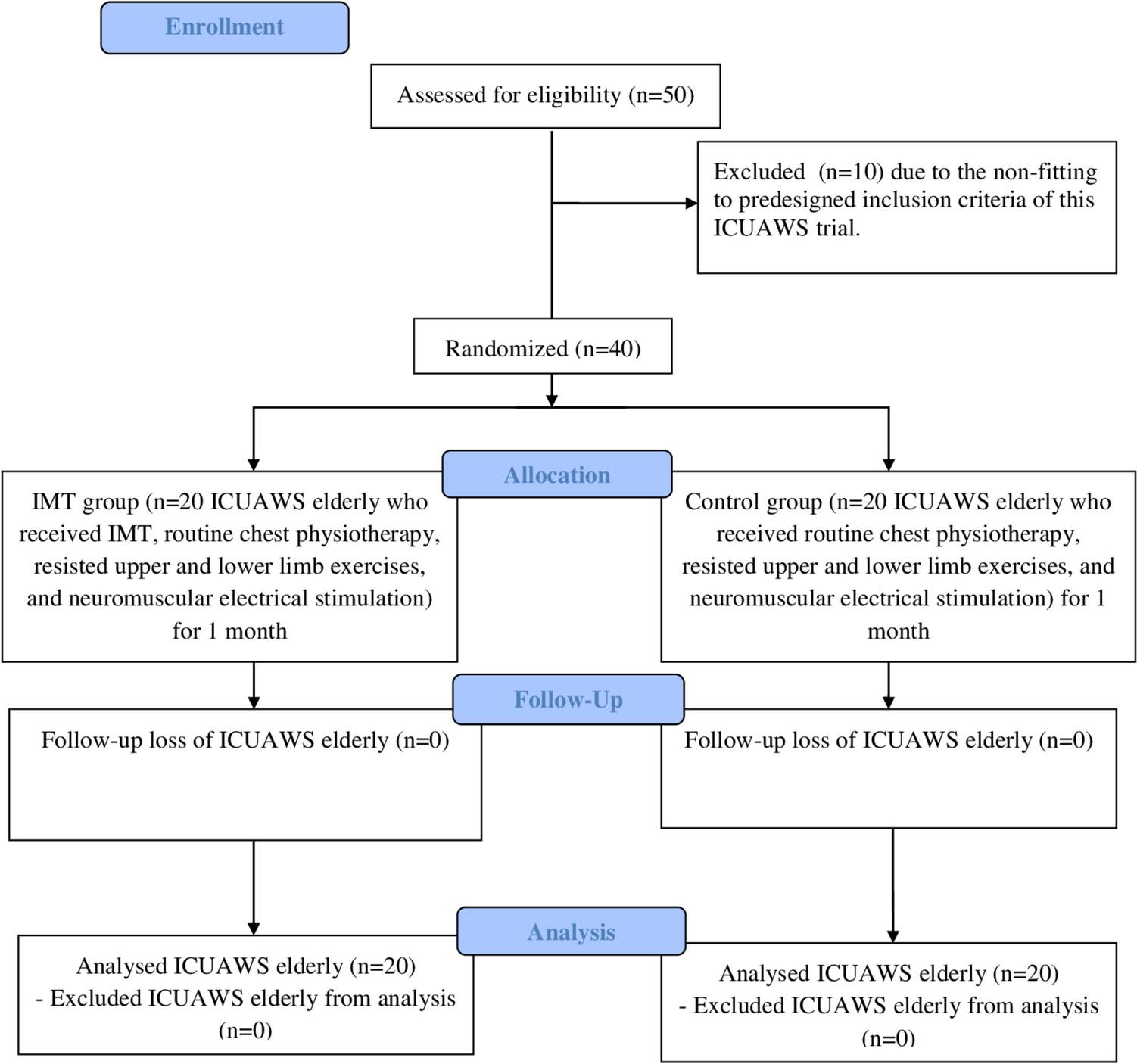
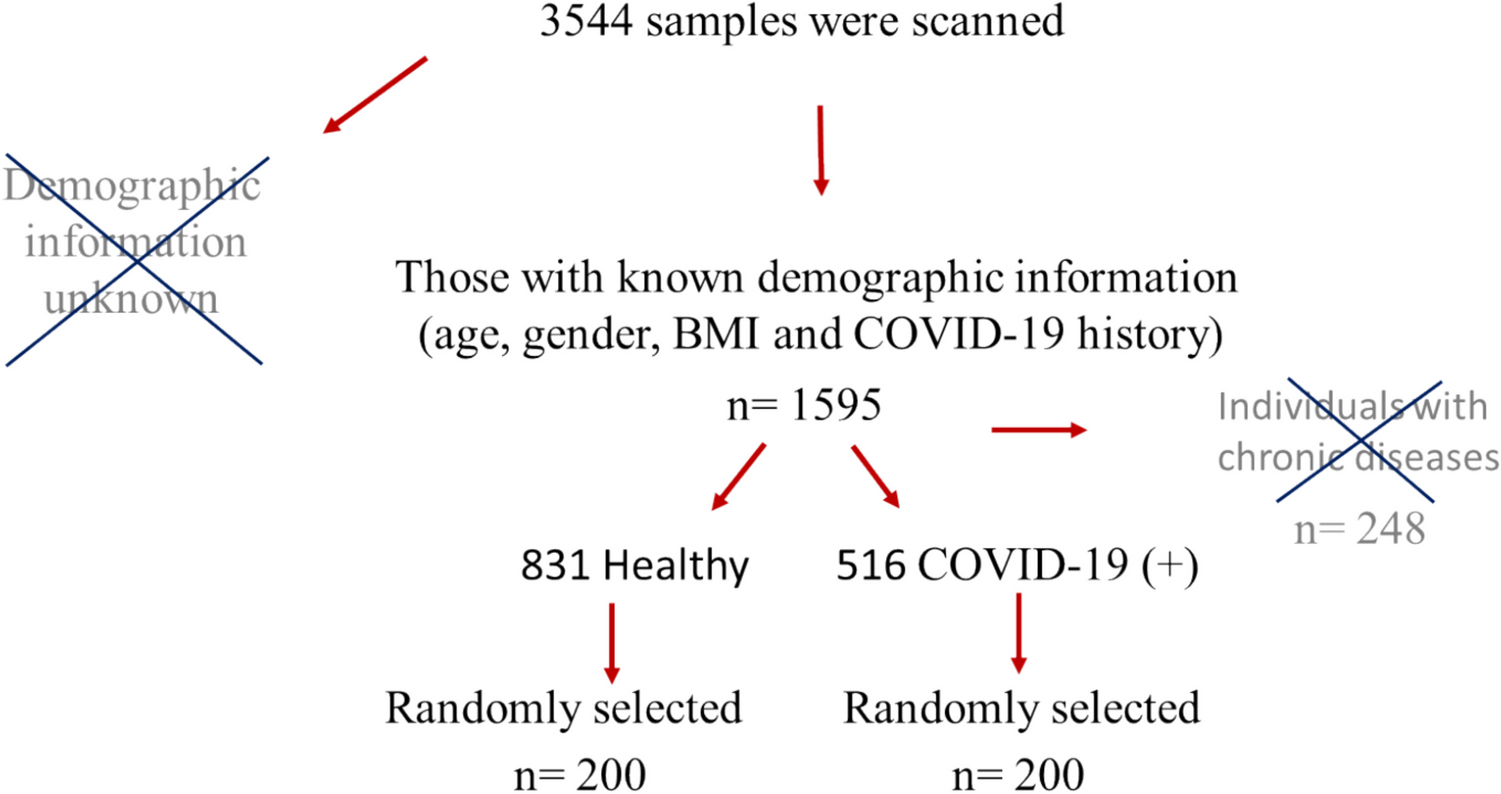
Study designIn this study, serum samples were obtained from individuals aged 18 to 60 who did not have any chronic diseases. Samples from individuals with chronic diseases or a history of autoimmune diseases were excluded from the study. To determine the prevalence of ANA following COVID-19, the population of Malatya province (approximately 800,000) was considered, and the required sample size was calculated to be n = 400. A total of 3,544 serum samples were collected during the pandemic period (between 2019 and 2022). Demographic information was unavailable for 1,949 samples, which were excluded from the study. Of the remaining 1,595 serum samples, those from individuals with chronic diseases such as asthma, diabetes, and autoimmune conditions were removed (n = 248). This left 1,347 samples, which were categorized into two groups: individuals who had contracted COVID-19 (n = 516) and healthy individuals who had not (n = 831). From each group, 200 samples were randomly selected using Excel’s random sampling function to create the experimental groups (Fig. 1). Thus, a total of 200 healthy individuals (100 men, 100 women) and 200 COVID-19 recovered individuals (80 men, 120 women) were included in the study.
Fig. 1
Determination of research samples. In the random selection process, samples were numbered and transferred to excel. The "RANDARRAY" function in excel was utilized to select 200 samples from both COVID-19 positive individuals and healthy controls
The criteria for COVID-19 diagnosis required the presence of at least one symptom (such as loss of taste, loss of smell, fever, etc.) and a positive PCR test and/or elevated SARS-CoV-2 antibody levels. Individuals who did not meet the diagnostic criteria established by the Ministry of Health and had negative antibody tests were classified as not having COVID-19.
The samples were analyzed using the ELISA method, and three distinct ELISA test kits were developed and validated for the measurement of ANA. Two of these tests, anti-dsDNA and anti-ENA, are widely utilized in both clinical practice and research literature. The third test utilized intact cell nuclei as the antigen. The Hep-2 cell line, commonly used in immunofluorescence assay (IFA) techniques and rich in ANA antigens, was selected as the source of nuclei for this test. By employing the Hep-2 nuclei, which contain various ANA antigens beyond dsDNA and ENA, we aimed to ensure that no positive ANA samples were overlooked.
Development of ANA ELISA test kitsThe calf thymus gland was utilized as the antigenic source for the dsDNA and ENA tests, while nuclei were isolated from the Hep-2 cell line. All three test kits were designed according to the indirect ELISA method. However, there were differences in the attachment of antigens to the well bottom. In the ENA test, the antigens were directly attached to the bottom of the wells in PBS, while in the dsDNA test, protamine sulfate was employed as a linker substance to bind DNA to the wells. In the Hep-2 nucleus test, nuclei were bound to the bottom using a commercial solution (Kementec, WellChampion) and subsequently blocked with this solution. 1% BSA was used for blocking in the dsDNA and ENA tests. Additionally, unlike the other two tests, in the Hep-2 nucleus test, Triton X was used to enhance membrane permeability, as intact nuclei were utilized. All subsequent steps were similar for all three tests. Serum samples were diluted 1/100 and added to the wells alongside negative and positive control samples. Subsequently, anti-human IgG conjugated with biotin and streptavidin peroxidase was added. Plates were washed three times with 0.05% Tween before each solution was added. Finally, a chromogenic substrate (tetramethylbenzidine, TMB) was added, and the reaction was halted with 11% H₂SO₄. The plates were then read using a spectrophotometer at 450 nm.
Validation of test kits: intra-assay and inter-assay dataThe intra-assay (within-test) and inter-assay (between-test) CV percentages were obtained by performing repeated measurements of two negative and two positive samples across four different plates. These values were computed using the formula: “% CV = (OD standard deviation / OD mean) × 100.” The intra- and inter-assay means for the dsDNA, ENA, and Hep-2 nucleus tests were 7.8%, 7.5%, and 9.9%, respectively.
Sensitivity and specificity analysisFor the sensitivity and specificity analyses, dsDNA and ENA positive and negative samples were analyzed at the İnönü University Medical Faculty Central Microbiology Laboratory (DIESSE Diagnostica Senese S.p.A. Chorus ds-DNA-G, ANA-8). For the dsDNA test, 48 positive and 48 negative samples were used, while for the ENA and Hep-2 tests, 12 negative and 12 positive samples were used. The positive samples used in the Hep-2 nucleus test were positive for both dsDNA and ENA. The sensitivities for the dsDNA, ENA, and Hep-2 nucleus tests were found to be 93.8%, 83.3%, and 90%, respectively, while the specificities for these tests were 91.7%, 83.3%, and 87.5%, respectively.
Cross-reactivity with different types of autoantibodiesSerum samples that exhibited negative ANA levels but tested positive for various autoantibodies (anti-cyclic citrullinated peptide (anti-CCP) [n = 2], anti-β2-glycoprotein I [n = 2], anti-myeloperoxidase (anti-MPO) [n = 1], anti-proteinase 3 (anti-PR3) [n = 2], and anti-cardiolipin [n = 1]) were analyzed to assess cross-reactivity in dsDNA, ENA, and Hep-2 nucleus testing. The results indicated that the five different autoantibodies examined did not exhibit cross-reactivity in the dsDNA and Hep-2 nucleus tests; however, anti-CCP and anti-β2-glycoprotein demonstrated low levels of cross-reactivity in the ENA test.
Sample analysisWhile the majority of the samples analyzed consisted of serum, a few samples were derived from plasma, and some were hemolyzed serum. Therefore, the impact of serum, plasma, and hemolyzed serum samples from the same individual on the test results was evaluated. The findings indicated that samples from all three types did not significantly affect the test outcomes.
ANA measurements were conducted using three validated ELISA test kits (dsDNA, ENA, and Hep-2 nucleus). The cut-off value was established based on the negative control optical density (OD) multiplied by 1.5, as determined in the validation studies. The obtained OD values were converted to an antibody index using the formula: Ab index = Sample OD / Cut-off OD. Samples with an index value of < 1.0 were classified as ANA IgG negative, while those with an index value > 1.0 were classified as ANA IgG positive. The test was considered valid if the antibody index of the positive control was > 1.1 and that of the negative control was < 0.9.
留言 (0)