
記住我
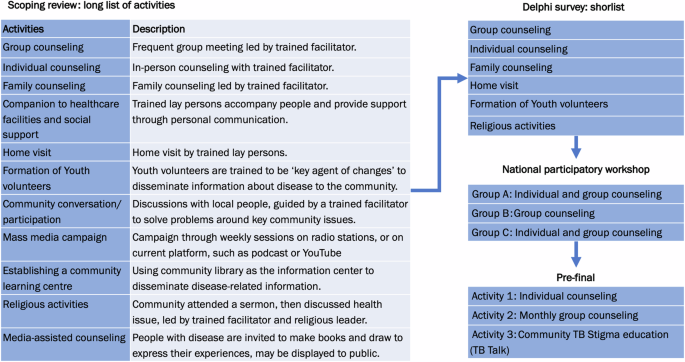




After screening 13,252 titles and abstracts, we selected 29 articles and reports for inclusion in the scoping review. From these articles, we found 12 discrete intervention activities that were perceived by the project team to have the potential to be incorporated into a complex community-based psychosocial intervention to reduce TB Stigma and depression among people with TB in Indonesia. The detailed results of the scoping review are reported elsewhere27.
Modified Delphi SurveyOf 25 persons invited to complete the modified Delphi survey, 22 participants (88%, 13 female and 9 male) completed the survey (Table 1). Three participants (a person with DS-TB, a member of the TB Civil Society Organization, and a District Health Officer) did not complete the survey, citing a lack of confidence in providing appropriate answers despite support from our team. These participants were happy to continue in other workshop activities. As planned, the participants represented diverse stakeholder groups: seven from civil society organizations including TB survivor organizations (Association of TB Patient Organizations), six from academics or researchers, five from the government (NTP, DHOs, and community health centre staff) and four people with TB (two with DS-TB and two with DR-TB).
Table 1 Participants in Delphi survey and national participatory workshop.From the survey, we shortlisted six activities for potential inclusion in the intervention package. The activities included: group counselling, individual counselling, family counselling, home visits, training and formation of youth volunteer cadres, and religious activities. These six shortlisted activities were further discussed in the participatory workshop.
National Participatory WorkshopThe national workshop was held a day after the modified Delphi survey. Two participants from the central government could not attend the workshop. The 20 participants were divided into three groups: A, B, and C. All groups agreed that psychological counselling to cope with stigma and/or depression should be included in the intervention activities, delivered either in a group or a combination of individual and group psychological counselling. Group A suggested a combination of activities: (1) at the individual level by delivering individual psychological counselling and home visit, (2) at the family level by delivering family counselling and a home visit, and (3) at the community level by providing peer group counselling with media-assisted education, such as video, and youth volunteer activities to deliver education on TB Stigma reduction. Home visits, in particular, were proposed to be applied at treatment initiation, at the completion of the intensive phase, and at the completion of the continuation phase for all people with TB.
These multi-level activities proposed by Group A were critiqued by groups B and C as being unfeasible and highly resource-intensive. Group B reported that they had selected a more pragmatic approach by recommending only peer-led group psychological counselling, citing this as “feasible for a relatively short period during the implementation study” and “not requiring high resources”. They went on to suggest that this peer group counselling should be implemented 3-4 times over the standard 6-month DS-TB treatment period. Group B reported that this recommendation was based on evidence that mutual support groups and group counselling (as opposed to individual counselling) were more effective to reduce self-stigma and anticipated stigma, which our previous research had identified as the most potentially modifiable forms of TB Stigma.
“Based on our previous discussions, the problems we want to address are self-stigma and anticipated stigma. Can we address TB Stigma in the community or other types of stigmas (by delivering meeting and counselling)? We need to better understand feasibility, to limit the [breadth] of problems [related to stigma] we intend to address, and to focus the intervention we develop on reducing self-stigma and anticipated stigma.” Group B representative.
Group C offered a combination of activities consisting of (1) healthcare facility-based counselling into TB treatment including adherence and adverse effects, while people attend a routine TB visit, (2) monthly group counselling, and (3) individual counselling (when a person is indicated as having a mental health disorder). They argued that providing only group counselling means that people who do not join the meeting, some of whom may potentially have substantial unmet needs for mental health support, will not be reached.
“(If we only provide group counselling) we cannot reach those who do not join the group counselling. Then we need help from Community Health Volunteers and TB Program Officers to identify and approach those who are not engaged (in the intervention) or do not adhere to the treatment, through medical and individual counselling.” Group C representative
During the discussion, it was also highlighted that the intervention should not focus only on reducing TB Stigma, but also depression and anxiety.
“Among those with a high level, or even a moderate level, of stigma, it can result in high levels of depression or anxiety (for which we have to intervene).” Group C representative
It was recommended by all groups that, once group psychological counselling was implemented, sessions should occur at least monthly, and people with TB would ideally join 2-4 group counselling during their first six months of TB treatment. However, there were debates on who should lead and facilitate the group counselling and the optimal location for meetings to take place. Group A suggested Community Health Volunteers (CHVs) as group counselling facilitators and that meetings take place in a healthcare facility. However, Groups B and C had different opinions, suggesting that, based on some of their members’ past experiences, healthcare facilities were “not a (physically) comfortable place”, “too cramped”, “close to a garbage dump”, or could “potentially lead to being recognized as having TB (by neighbours)” that “can lead to stigmatization”.
Group B suggested CHVs as the lead facilitators, together with TB program officers and TB survivors. This proposal was based on experience in conducting group discussions when people with MDR-TB can chat and share experiences, called a “super group”, held once in three months, led by MDR-TB survivors. The group discussions had been implemented for more than one year in several MDR-TB facilities, funded by an international donor. They found that TB survivors had challenges to successfully facilitate group counselling, resulting in suboptimal delivery and impact. A new intervention needs to complement the available resources in the community and avoid reinventing the wheel, by only assigning TB survivor as peer group counselling leader. However, assigning TB program officers as the leading group facilitator may “prevent people with TB from being open” to share their thoughts.
All groups agreed that training to become a group counselling facilitator was necessary and should be implemented in the preparation phase prior to leading group sessions. Based on experiences, despite the higher proportion of female group facilitators than male, “about 60% vs 40%”, there was no perceived difference in acceptability and impact of counselling sessions provided by female vs male facilitators.
A training module was discussed across groups as an important prerequisite to ensure that the facilitators are well-trained prior to intervention implementation. The groups mentioned key topics that should be incorporated into the core curriculum of any training module, including TB basic knowledge, TB treatment and its adverse effects, TB Stigma, nutrition, empathy, personal communication skills, and public speaking skills. Groups noted that there were many different and complementary modes by which these topics could be taught and learnt including lectures, role-playing activities, brainstorming, and interactive games.
At the end of the workshop, the pre-final intervention activities were formulated and updated during interactive discussions with all participants (Fig. 1). This consisted of three activities. Firstly, individual counselling by either healthcare workers or research team members applied at the first healthcare visit following a TB diagnosis. At this point, the baseline status of people with TB’s stigma levels, mental health, and quality of life will also be evaluated using tools validated in the Indonesian setting7,12 and a verbal and written invitation to a group psychological counselling will be provided. Secondly, a monthly community-based group counselling will be held in an agreed communal space distinct from healthcare facilities and led by TB survivors. Thirdly, a community activity, such as TB talks, will be held to improve community knowledge about TB and reduce TB Stigma in community, by inviting people with TB and their families to lead the talks and share their experiences to the public or neighbouring communities.
Fig. 1: Co-development stages to select psychosocial intervention activities.
Development of the intervention activities from scoping review long-list to participatory workshop Group short-list, to selected pre-final intervention activities.
An important point that arose during the meeting was that people with TB participating in the workshop voiced in open discussion sessions that they felt that their experiences and perceptions were being addressed and that they were being listened to during the co-development process.
“I didn’t ever realise that I could actually say out loud what I need as someone with TB. I have just realized that this happens now.” Male participant with DS-TB, currently receiving treatment.
“This is what I have been waiting for for a long time. I really wish that my friends, people undergoing drug-resistant TB treatment, could have people or someone, with whom they can share their feelings…” A female participant and DR-TB survivor.
Finalization of the InterventionThe pre-final intervention activities were then discussed internally amongst the research team. In this phase, we did not exclude any activities agreed upon in the workshop. Rather, based on the feasibility of these activities, we shaped the potential implementation strategy of the intervention, including the timing of activity delivery and delivery personnel including counselling providers opted to include the individual psychological counselling at the first healthcare visit to assess the acceptance to TB diagnosis, the readiness for TB treatment, and the stigma and mental health people with TB experience. This psychological counselling may also avoid “rational non-adherence”, when people with TB, feel that they cannot continue the treatment because of reasonable factors they face in their life, healthcare worker advice, or adverse effects—a phenomenon which was also found among people with HIV/AIDS31.
“The current approach is that we want people with TB to take the treatment as soon as they are diagnosed. Once the sputum test gives a positive result, they have to start treatment directly, without assessing their readiness…. It is better to build a strong foundation (upon which people with TB accept the diagnosis and are ready for TB treatment). If they are ready, they will not discontinue the treatment.” Psychologist
With regards to leadership of the group counselling and learning from the reported challenges of leadership by people with TB alone, especially if training is not adequate, we opted for integrated leadership and facilitation shared between TB survivors and general practitioners. We opted for TB survivors to be accompanied by general practitioners instead of TB program officers, who were reported by one stakeholder to be “overwhelmed with their work burden at healthcare facilities”, or CHVs, who may have a “perception of being in a more legitimate position than people with TB”, both potentially leading to a suboptimal counselling process. The peers, in addition, can still provide individual support through personal contact and group communication through a user-friendly communication platform, such as WhatsApp or other related platforms.
“Based on experience, many people want to become CHVs because CHVs are perceived as occupying a legitimate social position in their community, and not necessarily because they want to accompany people with TB. I observed in X (mentioning a district name), people with TB were only ordered, even scolded, by CHVs, and it may increase stigmatization.” Psychologist
At finalisation, the intervention activities consisted of (1) individual counselling and initial psychosocial assessment, (2) monthly group counselling facilitated by peers/TB survivors and general physicians, (3) personal contact and group communication facilitated by peers/TB survivors, (4) TB Talks, a public education talk inviting all people in neighbouring communities, where TB survivors, people with TB, and their families share their experiences with the general community, along with public education about TB and stigma by healthcare workers and (5) evaluation. (Fig. 2)
Fig. 2: Final psychosocial intervention activities selected to be evaluated in the TB CAPS Study.
Final intervention activities for the TB CAPS Study.
留言 (0)