
記住我
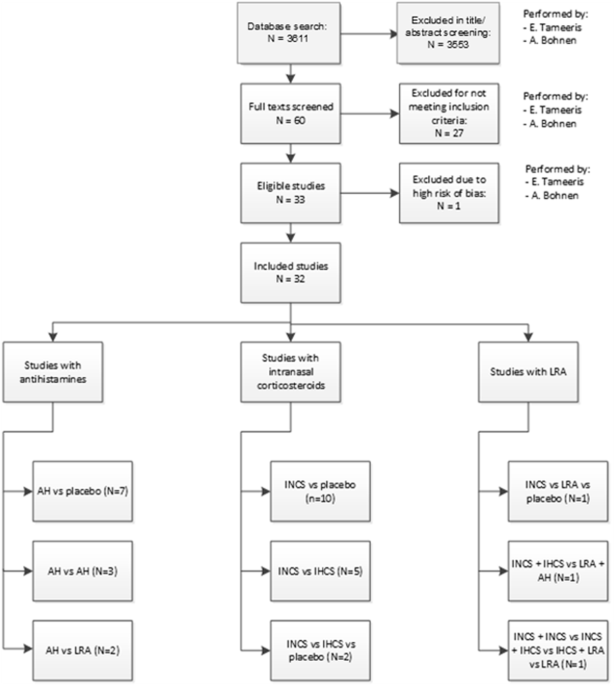






The search was performed and updated up to October 2024. In total, 3762 unique publications were retrieved. After title and abstract screening, 60 articles remained for full-text assessment. 33 articles were included in this review. One article was assessed as high risk of bias and was excluded. The primary reasons for exclusion in the full-text assessment were: no asthma diagnosis (n = 7), no conventional medication studied (n = 7), no AR diagnosis (n = 4) (Fig. 1).
Fig. 1
Flowchart of the inclusion process.
The included studies were published between 1988 and 2018. Seven studies compared AH to placebo24,25,26,27,28,29,30, of which one used intranasal AH27. Ten compared INCS to placebo31,32,33,34,35,36,37,38,39,40. Three studies compared AH41,42,43 and two AH in addition to LRA44,45. Five studies compared INCS to IHCS46,47,48,49,50 and two studies INCS to IHCS and placebo51,52. The use of INCS was compared to LRA and placebo in one study53 and another study compared combined INCS and IHCS with LRA and AH54. One study compared the use of INCS alone with a combination of INCS and IHCS, a combination of INCS and LRA, and LRA alone55. The study investigating intranasal AH reported no statistically significant outcomes27.
Of the 32 studies included in this review, three had a crossover design34,47,54. The number of included patients varied from 12 to 1385. In total, 5987 patients were studied. Six studies had a paediatric study population (participants <18 years old)26,34,37,39,43,46 and the population of 16 studies was partly paediatric28,29,30,31,32,35,41,44,45,48,49,51,52,53,54,55. Of the 33 studies, 16 performed measurements during the pollen season24,27,28,29,30,32,33,35,36,41,42,44,45,50,51,52. The intervention time in the reviewed studies varied from two to 26 weeks. Outcome measures are reported in Tables 2–4. An overview of the clinical symptom scoring methods used in the reviewed studies can be found in Supplementary Table 8.
Table 2 Overview of studies using antihistamines for allergic rhinitis in asthmatic patients.Table 3 Overview of studies using INCS for allergic rhinitis in asthmatic patients.Table 4 Studies using LRA for allergic rhinitis in asthmatic patients.Subjective asthma outcomesSubjective asthma outcomes were reported in 29 studies24,25,27,28,29,30,31,32,33,34,35,36,37,39,40,41,42,43,44,45,46,48,49,51,52,53,54,55,56. Most studies used an asthma symptom scoring system, allowing patients to log symptoms in a diary on a point scale (most commonly 0–3 points per symptom; see supplementary table 1 for specifications of the scoring systems).
AntihistaminesOf the studies investigating AH, 11 reported asthma symptom scores (ASS)24,25,27,28,29,30,41,42,43,44,45,57. Nine studies found a significant improvement, the clinical relevance of these improvements is not described. There are no differences in outcomes between studies performed during the pollen season24,27,28,29,30,41,42,44 and those performed outside the pollen season45. Tinkelman et al. (1996) performed their study on an exclusively paediatric population43. Nathan (2006), Pasquali (2006) and Balzano (1992) had an exclusively adult study population. No differences were seen in the subjective asthma symptoms for the different study populations. Nathan (2006) measured the QoL with the Asthma Quality of Life Questionnaire (AQLQ), which resulted in a significant improvement from 4.4 to 3.5. The minimal important within-subject change in the AQLQ overall score is 0.5, and the reported improvement is considered moderate21,24. Pasquali (2006) measured the RHINASTHMA global summary (GS) score, which improved from 28 to 16 in the levocetirizine intervention group, versus an improvement from 31 to 27 in the placebo group25.
Intranasal corticosteroidsFourteen studies described the effect of INCS on reported ASS31,32,33,34,35,36,37,
留言 (0)