Study type and study period
We performed retrospective descriptive analyses of AMR pathogen incidences before and during the COVID-19 pandemic, analysing CRA, MRSA, CRKP and CREC. Starting with the introduction of the notification requirements, our study period included complete weeks between 2 January 2017 (only MRSA: 5 January 2015) and 25 December 2022. We specified pre-pandemic (01/2015–12/2019) and pandemic (01/2020–12/2022) periods. Although Germany initially reported cases in February 2020 [10], we included the whole year as pandemic period to obtain comparable annual intervals.
Primary study database, study population and case definitions
Our main database was the German statutory notification surveillance system, which records mandatory CRA, CRKP, CREC and invasive MRSA notifications by laboratories according to § 7 Infection Protection Act (IfSG) [6]. The study population included cases fulfilling § 11 [2] IfSG [6, 17] case definitions, with notification date in the study period. Cases were defined as individuals with newly detected CRA, CRKP and CREC infections or colonisations with a carbapenemase or reduced phenotypic sensitivity. MRSA cases were defined as new Staphylococcus aureus infections in blood or cerebrospinal fluid with mecA-gene detection or phenotypic methicillin resistance.
We included COVID-19 cases in Germany according to the statutory case definition [17], along with population data and annual hospital inpatient counts from the German Federal Statistical Office (DESTATIS) [18].
Secondary study database, study population, and case definitions
We used the Antibiotic Resistance Surveillance (ARS) as our secondary database [19]. ARS is a laboratory-based surveillance network comprising data of about one third of German hospitals. Results of their routine antibiotic susceptibility testing are voluntarily transferred by respective laboratories to the Robert Koch Institute.
Analogous to statutory case definitions, we considered isolates resistant upon classification as resistant (“R”) or susceptible upon increased exposure (“I”) to imipenem or meropenem for CRA, CRKP and CREC and resistant (“R”) to oxacillin or flucloxacillin for MRSA. Between 2017 and 2022 we included the first isolate per patient per quarter (copy-strain-rule) from laboratories that participated in ARS throughout 2017–2022. We excluded screening isolates.
Data and descriptive epidemiology
The following information was available for notifications: pathogen, notification date, age, federal state, infection/colonisation, mobility history, hospitalization date(s), sample date(s), sample material(s), death, if cases belonged to an outbreak, and outbreak setting.
We considered cases with pathogen detection in blood, cerebrospinal fluid, bronchoalveolar lavage, urine or wound samples as infected, and cases with detection in stool or screening samples as colonised. We defined the presumed acquisition setting based on a combination of statutory variables: infection/colonisation, mobility history, hospitalisation date(s), sample date(s), sample material(s), outbreak involvement and outbreak setting. We distinguished “probably nosocomial”, “possibly nosocomial”, “possibly community”, “possibly international” and “missing”.
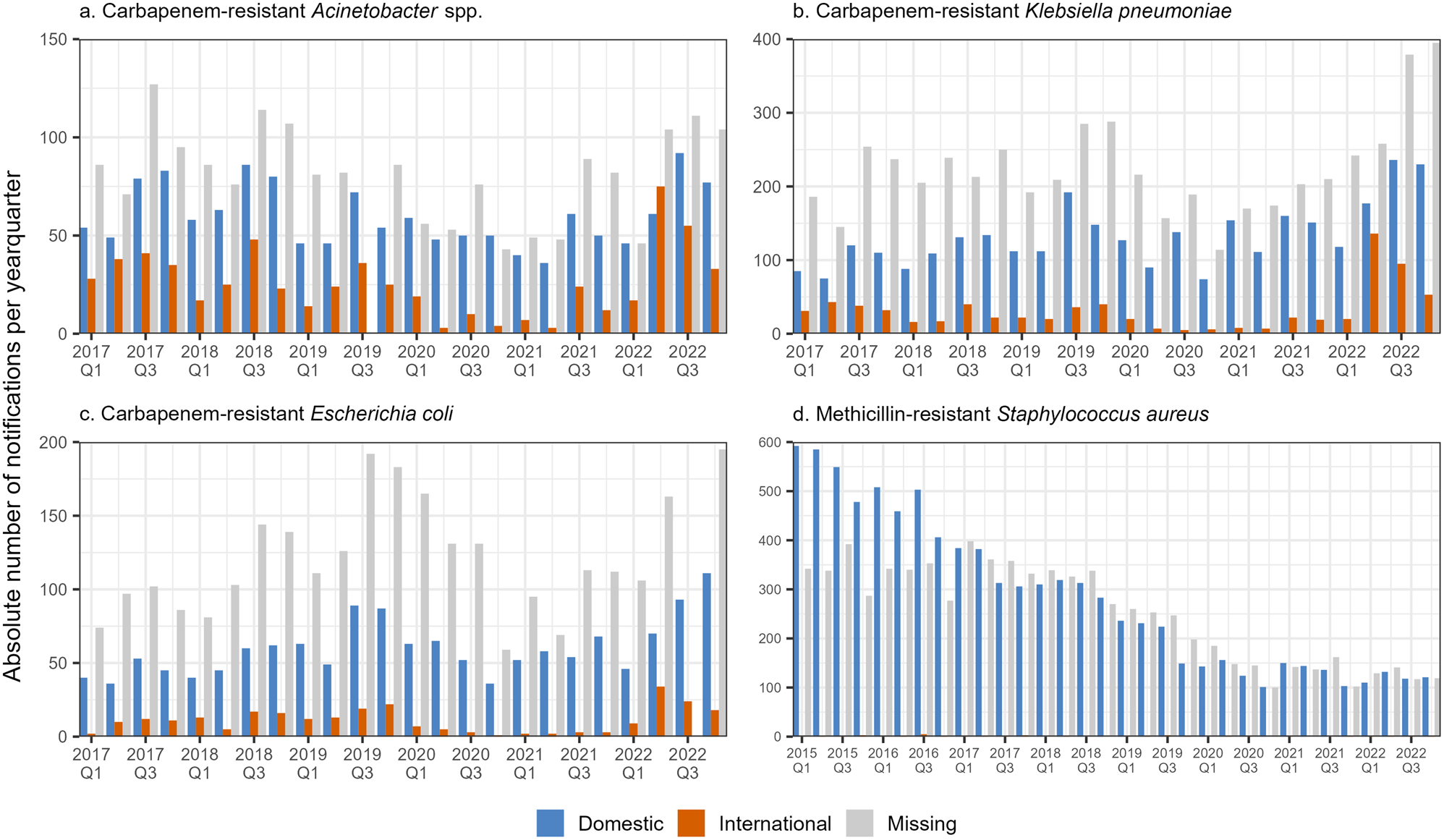
We categorised mobility history into “domestic”, “international“ (i.e. at least one international stay possibly relevant for exposure), and “missing”. To analyse international mobility, we selected the top five reported countries per CRA, CRKP and CREC. For CRKP less frequent countries were grouped as “other”. We excluded MRSA from this sub-analysis due to the limited number of documented prior international stays.
We described notified cases by monthly incidence, sex and age groups, federal states, infection/colonisation, acquisition setting, outcome death (for infected cases only) and (international) mobility in pre-pandemic and pandemic periods. Due to varying case definitions, we excluded MRSA from sub-analyses regarding infection/colonisation and acquisition setting. Moreover, we plotted weekly pathogen counts and SARS-CoV-2 notifications together.
For ARS isolates, we analysed pathogen, date, copy-strain-rule, care type, sample material and results of resistance testing for imipenem and meropenem (CRA, CREC, CRKP) or oxacillin and flucloxacillin (MRSA). We identified isolates from infections based on the sample material types blood culture, respiratory, punctate, urine or wound.
Statistical analyses and modelling
To quantify changes in incidence before and during the pandemic, we (a) fitted regression models that reflected observed annual incidences throughout the study period (2015/2017–2022), (b) used these to project annual incidence in the pandemic period (2020–2022) while assuming pre-pandemic trends continued, and (c) compared observed with projected incidence rate ratios (IRR) per pandemic year. We interpreted them as relative changes, i.e. as relative reductions (negative values) or increases (positive values) of observed incidence relative to hypothetical projections. We modelled the hypothetical annual incidences in the pandemic years by: (a) building the regression models based on the entire study period with a dummy covariate that was 0 for pre-pandemic and 1, 2 or 3 for pandemic years and (b) re-running the regression models with the dummy covariate set to 0 for all years (Supplementary Text 1). 95% confidence intervals (95% CI) and p-values (p) below 5% indicated statistical significance.
We employed 4 modelling approaches: In a primary annual model, we fitted Poisson or negative binomial regression models to annual case numbers and assessed them based on likelihood-ratio-tests. A second annual model additionally accounted for the concurrent reduction in hospitalization by including hospital inpatient numbers as an offset. To reflect pathogen seasonality and sub-annual trends, a third weekly model in an interrupted time series analysis design was fitted to weekly notifications. We used Poisson regression for baseline trend and sine/cosine terms for seasonality, informed by periodograms of weekly notifications. As before, an additional fourth weekly model accounted for the concurrent hospital inpatient count (Supplementary Text 1).
With ARS data, we employed the primary annual models for all isolates, resistant isolates, resistant isolates from infections only and resistant isolates stratified by inpatient or outpatient care type. We also analysed the percentage of resistance, relative to all isolates.
We compared sociodemographics and assessed changes in the distribution of categorical variables between the pre-pandemic and the pandemic period 2020–2021 using the chi-squared statistical test. For this analysis we excluded 2022 from the pandemic period due to relatively different AMR trends.
Statistical software
We used R (4.2.2) [20] and RStudio (2023.03.0.B.386) [21], including packages tidyverse, lubridate, ISOweek, tsibble, MASS, trending, lmtest, TSA, slider, ggalluvial, ggh4x, RColorBrewer, gtsummary and flextable.





留言 (0)