Our study reports the normative coronal dimensions of the FN on fs-gad T1-weighted MRI, while also investigating its relationship with age, sex and ONS size. This study is the first to present normative FN measurements across any imaging modality. Additionally, we utilised high-resolution MRI scans in over 160 orbits. These findings may aid in defining a quantifiable definition for FN enlargement.
The upper ranges of the FN measurements, set at two standard deviations above the mean, could serve as a suitable criterion for defining the threshold of FN enlargement. Two standard deviations above the mean diameter were chosen to define abnormal enlargement [4, 13]. A diameter greater than 1.1mm in the coronal plane for the FN may be considered enlarged. Current definitions of enlargement require the FN’s diameter to be greater than that of the ONS, which is around 5mm. Our proposed normative data suggests that this criterion may under report the prevalence of FN enlargement.
One previous study measured the size of an enlarged FN, reporting dimensions of 20.6mm × 31.8mm [21], however no previous studies have reported the normative values. Therefore, a quantitative cut-off for FN enlargement has yet to be established. In our study, the FN and ONS measurements were taken at its maximum diameter as this can be used to help define abnormal enlargement [19]. The infraorbital nerve is the most common trigeminal branch lesion associated with IgG4-ROD [3, 18, 20], and its involvement is a prognostic indicator of IgG4-ROD and correlates with serum IgG4 levels and occurrence of multi-organ involvement [21]. Further studies may investigate if frontal nerve enlargement, defined using our normative data, may also serve as a marker of disease severity in IgG4-ROD.
Our study found no significant difference in FN diameter with respect to age group, sex, or laterality. Further studies across different centres are required to corroborate our findings. In addition, data on the ethnicity of the participants, which was not available in our study, would also be helpful to see if the diameters vary across different ethnic groups.
As current definitions define FN enlargement in relation to ONS size, this study provides the normative values for the FN:ONS ratio in both orbits. Given nerve size variability among individuals, the FN:ONS may be used as another quantitative indicator of FN enlargement. There was no significant difference in the FN:ONS between age groups or sex.
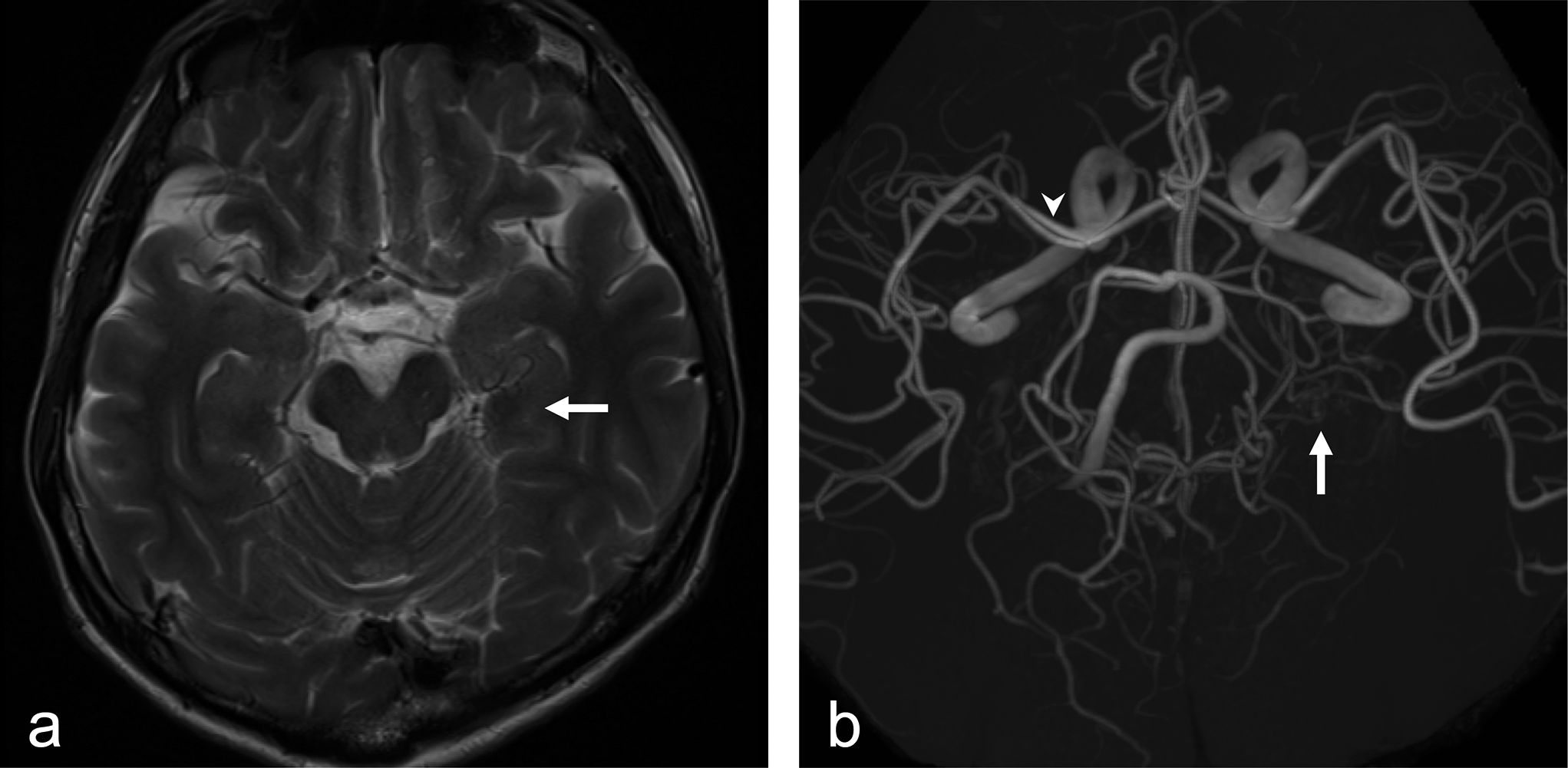
Coronal fs-gad T1-weighted MRI is the preferred imaging sequence for evaluating inflammatory and neoplastic conditions of the orbit. High-resolution volumetric T1-weighted images post-contrast enables for visualisation of trigeminal nerve branches. The frontal nerve is surrounded by a venous plexus which enhances, with the frontal nerve itself being relatively hypointense. Additionally, as the peripheral segments of the trigeminal nerve are surrounded by fat, employing fat-suppression sequences allow for clearer delineation of the FN [2]. Utilisation of high-resolution orbital MRI scans on 3T scanners allowed identification of the nerve in majority of cases (84/89 patients). However, five cases had unclear boundaries on two reviewers, including a neuroradiologist (SP) and therefore were excluded. MRI sequences with lower spatial resolution (e.g., 1.5 T) may see a higher proportion of cases where the boundaries of the frontal nerve may not be able to be distinguished.
Other causes of FN enlargement include adult-onset xanthogranuloma [14], lymphoma [9], schwannoma [21], idiopathic orbital inflammation, and neoplastic perineural spread from squamous cell carcinoma [12]. All of these cases had reported unilateral enlargement of the FN and are much less common than IgG4-ROD. The presence of bilateral trigeminal branch enlargement is specific for patients with IgG4-ROD [9, 17], with an approximate prevalence of 53% [9]. Therefore, the establishment of the normative diameter of the FN, along with the ability to assess bilateral FN enlargement on MRI, may help facilitate diagnosis of IgG4-ROD.
This study has limitations apparent in its design. The study is retrospective, based on patients from a single cohort which may not be applicable to other population groups.
Furthermore, this study did not comment on the shape of FN when measuring its diameter. In addition, frontal nerve and optic nerve sheath diameter may vary across its course and future studies could look at its dimensions at different points in its course.
In conclusion, we present the normative FN diameter in an Australian cohort using the fs-gad T1-weighted MRI. The data provides a cut-off of values that can be used to quantitively diagnose FN enlargement.









留言 (0)