The study participants in our review positively evaluated SIVR. However, SIVR has not shown better educational effectiveness than interactive non-SVR. Of the studies that involved non-stereoscopic images, four comprised desktop-based models [2, 11, 12, 25], and two involved immersive environments [20, 28]. It should be noted that the term “non-SVR” was not homogenously perceived in our review studies. In the papers by Wainman et al. [28] and Luursema et al. [20], this term meant “IVR without the ability of stereoscopic vision”. In the studies by de Faria et al. [12], Copson et al. [11], Patel et al. [25], and Barbara et al. [2], the term “non-SVR” was perceived as “desktop-based digital models.” Although those desktop-based models were projected on a 2D screen, they provided the ability of 3D perception. Thus, they could not be considered conventional 2D images (such as a PowerPoint presentation).
All the studies that compared SVR with non-SVR in terms of effectiveness involving interaction with the VR environment [11, 12, 20, 25] did not find significant differences. This finding contrasts with the meta-analysis by Bogomolova et al. [3], which showed that stereoscopy plays a critical role in the effectiveness of anatomy education when the 3D digital stereoscopic environment is interactive. However, this meta-analysis investigated the role of stereopsis in anatomy teaching in 3D visualization technologies without focusing on VR. More recent research by Bogomolova et al. [4], which compared stereoscopic augmented reality with non-stereoscopic teaching methods, also demonstrated that the former is not a more effective anatomy teaching tool. The meta-analysis by Bogomolova et al. [3] found that if stereopsis was combined with interaction, it was significantly more effective than in monoscopic 3D digital environments. In contrast, when interaction was absent, stereoscopic 3D visualization was not significantly more effective than monoscopic 3D one. Of note, in all studies of our review that involved interaction, SVR was not considerably superior to monoscopic digital images. In contrast, in the only study of the review that showed the superiority of SVR to monoscopic VR (MVR) [28], there was no interaction. In the same survey, stereopsis did not lead to better teaching effectiveness than critical 2D views of anatomical structures, while it was significantly inferior to physical models. There was no explanation for this difference in the educational outcomes of SVR. The fact that both forms of VR were found inferior to physical models and equally effective with critical 2D views can probably be explained by the absence of interaction between the users and the VR environment because interaction plays an important role when VR is used for anatomy teaching [8]. Only two papers explored the use of non-interactive SVR [19, 28]. Thus, there is insufficient data to evaluate this type of VR delivery.
In our review, three studies [11, 19, 28] showed that SVR was less effective than conventional 2D images. In one of those studies [11], the users interacted with the VR environment, while in two studies [19, 28] they did not. In contrast, de Faria et al. [12] demonstrated that SIVR led to significantly better outcomes than 2D images. These data do not show if interactive and non-interactive SIVR are more effective anatomy teaching tools than 2D images. Also, in the meta-analysis by Bogomolova et al. [3], it was unclear if stereopsis led to superior educational outcomes of 3D visualization compared to 2D images. Bogomolova et al. [3] showed that non-interactive stereoscopic images were less effective than 2D images.
Furthermore, in all studies of our review with evaluation of participants’ perceptions [2, 6, 11, 19, 25], SVR was considered more effective than traditional 2D methods or simply effective. However, it should be noted that the possible exposure to VR before the educational intervention might have influenced the participants’ perceptions of this technology. The studies of our review did not evaluate the effect of this possible exposure. The considerable acceptability of SVR indicates that this method has a non-ignorable potential in anatomy education. Thus, further research could enhance the academic performance of students taught via SVR environments. However, in all studies of the review assessing the side effects of the use of SVR [2, 12, 25], those effects were met considerably more frequently compared with other educational methods. Those side effects included nausea, dizziness, eye strain and discomfort. This fact raises concerns about whether SVR should be more widely applied. Currently, there is no data about which VR exposure duration is safe to avoid side effects.
The findings of our review have implications for several fields of health sciences where SVR has been applied. The implementation of this technology in health sciences has shown conflicting outcomes. Al Ali et al. [1] compared the impact of stereoscopic versus non-stereoscopic vision on dental students’ performance in a VR simulator. It was found that the former type of vision led to better depth perception and significantly impacted tooth-cutting accuracy within the target area. However, the stereoscopic view did not considerably influence the task completion time [1]. In another study [5], neurosurgical residents were trained in three procedures via SVR, and afterward, they completed a questionnaire to evaluate the use of this technology. Over nine out of ten participants stated that the educational intervention was helpful in their training, while the sickness due to the use of SVR was negligible [5]. Also, Vrillon et al. [27] investigated the use of this technology for medical students’ and residents’ lumbar puncture training. They found that the perceived benefit was high, while the discomfort was minimal. Despite the relatively positive perceptions about using SVR for health sciences training purposes, there is generally a lack of data regarding its educational effectiveness in the clinical setting. Although there is evidence that VR can not only improve residents’ skills but also be successfully applied in the operating room and enhance athletic training performance and injury rehabilitation [13], it has not been clarified in the literature if stereoscopic delivery is crucial for the value of VR in any health sciences domain. A wide variety of medical procedures [14, 17, 21, 24, 26], which have generated controversy regarding their outcomes, may benefit from the VR implementation; thus, the addition of a stereoscopic component may stimulate further research to shed light on the role of this component in the advantages of VR.
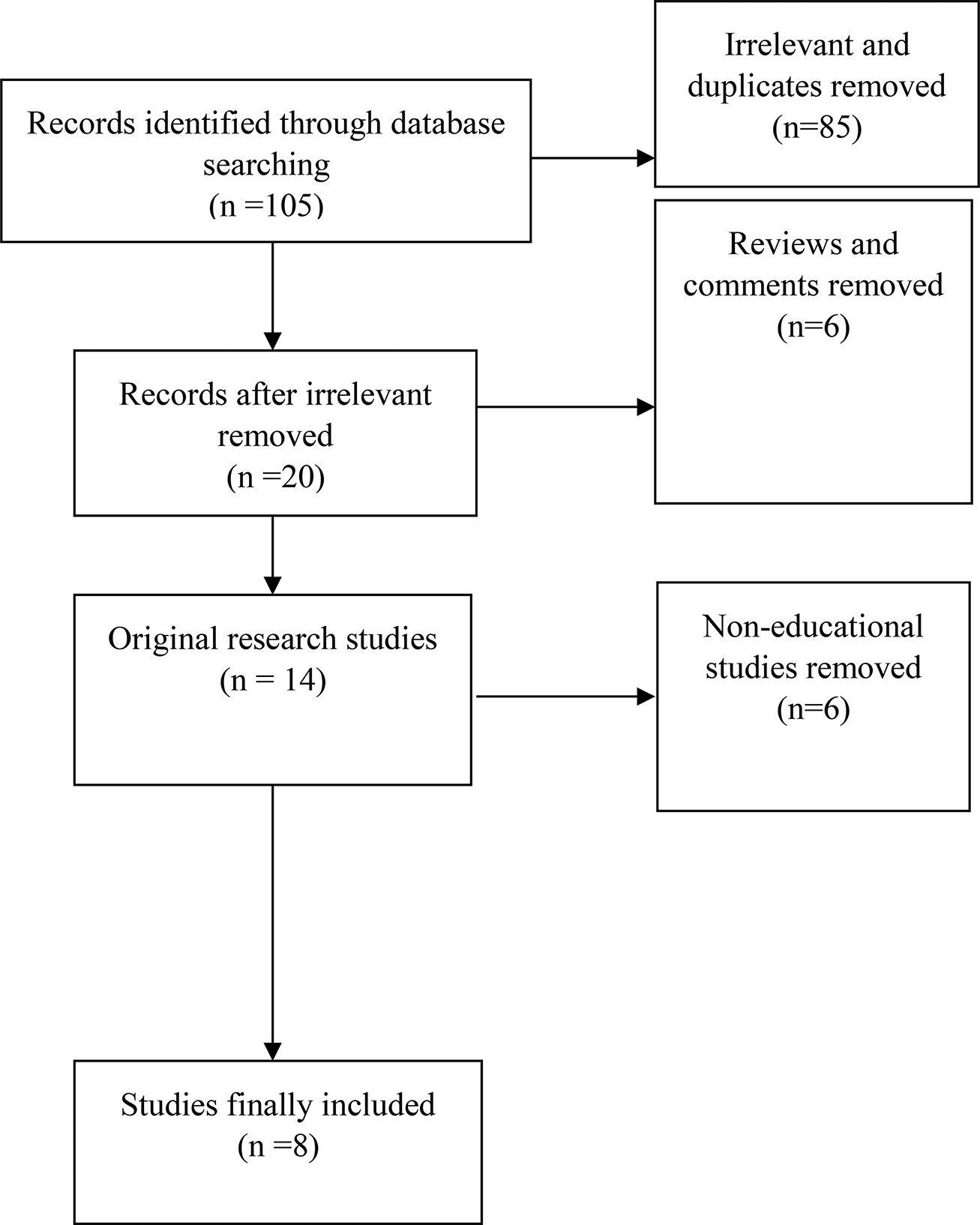
Our review does have some limitations. The included studies are relatively few, and the data is quite heterogeneous. Nevertheless, our literature search strategy has probably allowed us to include the maximum possible number of papers. We are optimistic that future research will produce more consistent and comprehensive data, facilitating a thorough meta-analysis.









留言 (0)