
記住我
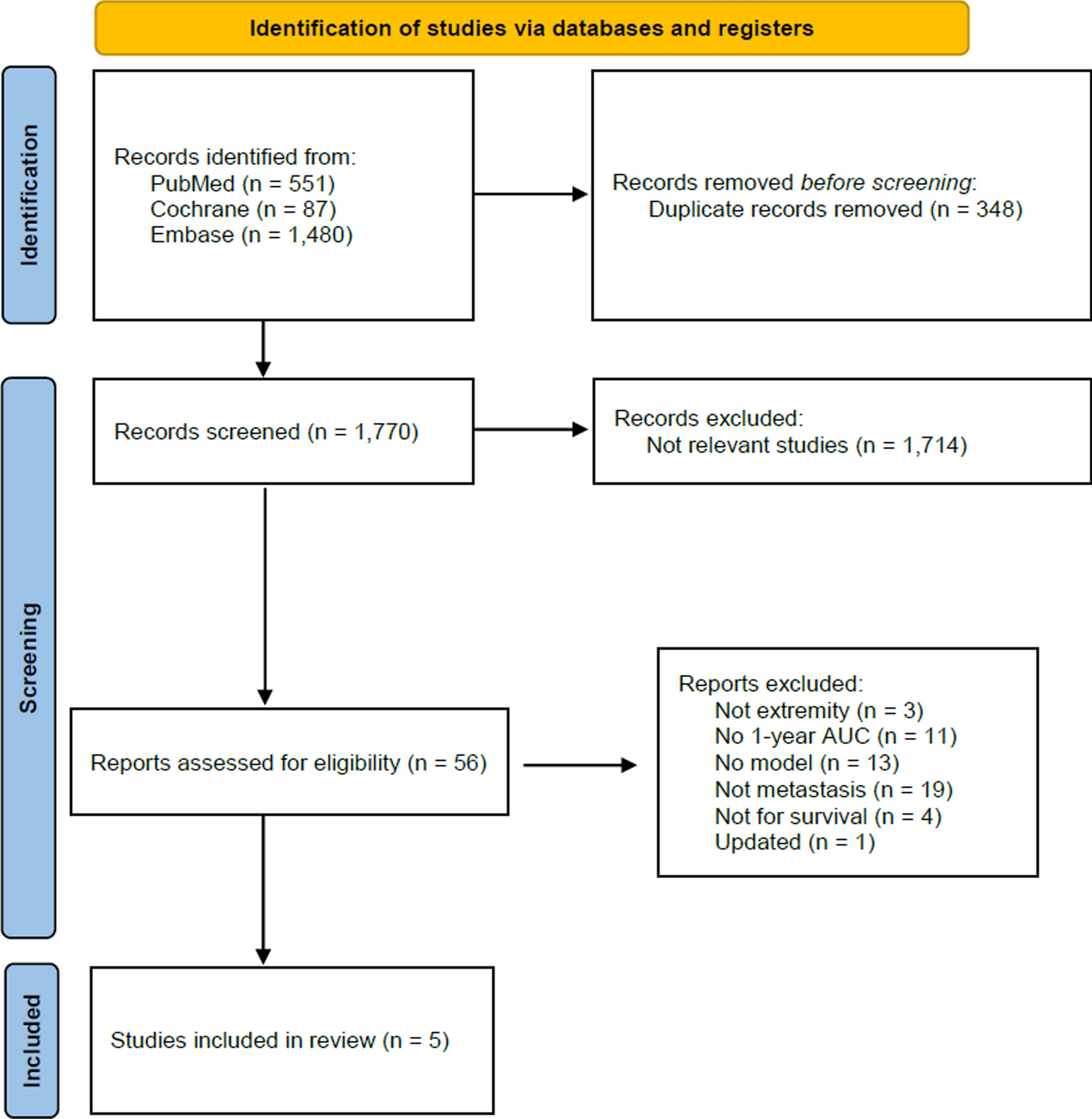






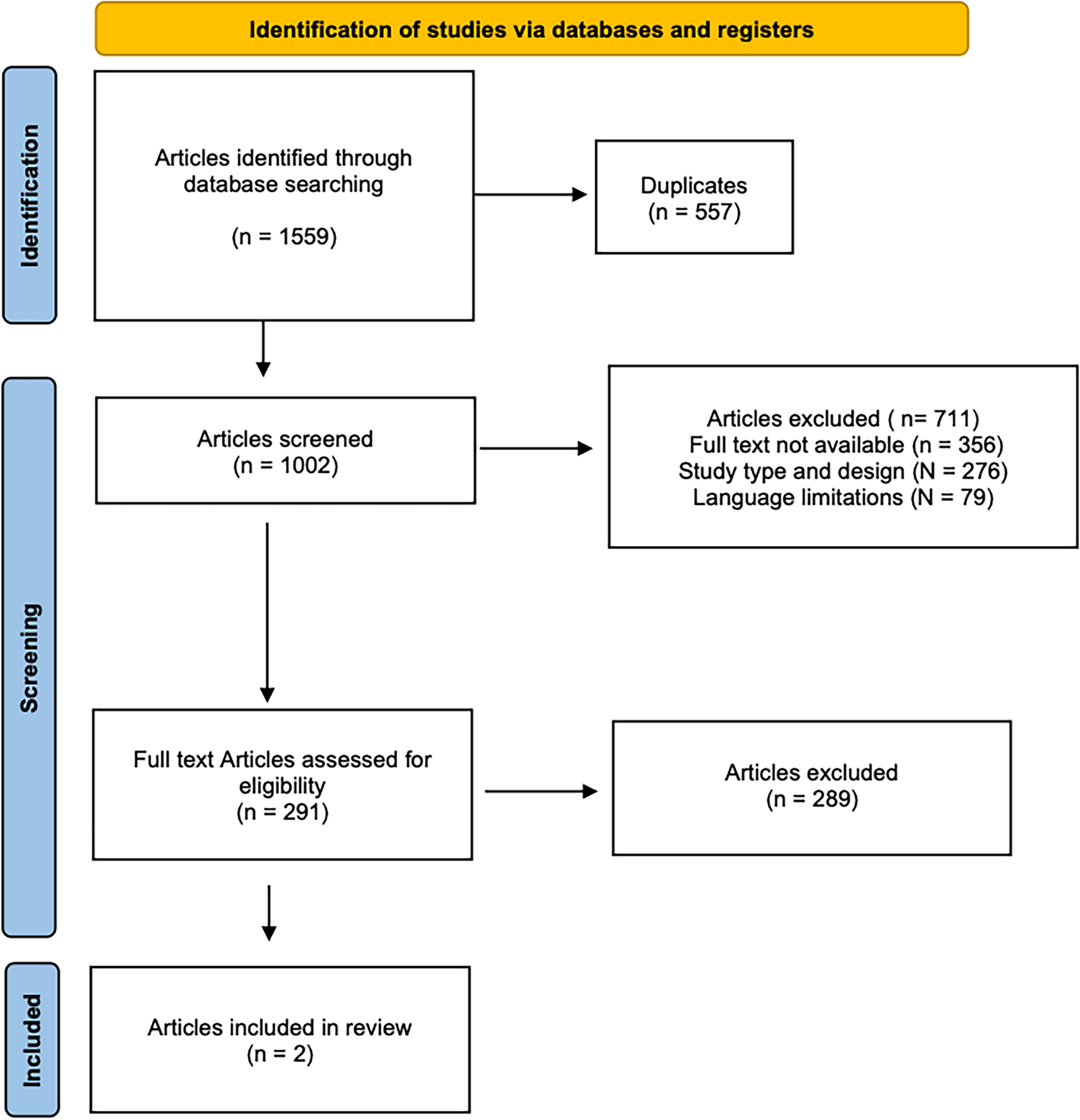
The study selection process is summarized in Figure 1 using a PRISMA flow diagram. The initial search yielded 1524 articles. After removing duplicates, a total of 1044 records remained. Based on the title and abstract, 943 studies were excluded as they were deemed irrelevant to this study. The remaining 101 papers were assessed in detail to verify their alignment with the inclusion criteria. After full-text screening, a total of 15 studies met the inclusion criteria.
Fig. 1
PRISMA flowchart showing the search for and selection of articles
Quality assessment of studiesAll selected studies were retrospective case series of a medium-to-small size (sample size = 3–32) that reported the outcomes of using the Masquelet technique in the long bones of the upper limb.
The manuscripts were published between 2014 and 2023. According to the MINORS scoring system, one study scored 6/16 points, two studies scored 7/16 points, two studies scored 8/16 points, four studies scored 9/16 points, two studies scored 10/16 points, three studies scored 11/16 points, and one study scored 12/16 points (Table 1).
Table 1 List of included studiesCohort characteristicsThe studies included 156 patients (Table 2) with a mean age of 42 years (ranging from 1 year to 79 years); the mean follow-up was 48 months (5–144 months).
Table 2 Summary of resultsEtiology and site of injuryThe patients included in the studies had bone defects due to both septic and aseptic causes. Of the 156 patients, 108 (69%) had septic lesions, while 48 (31%) had aseptic lesions. The initial cause of the bone defect was not always described. In the nine studies where it was described (totaling 89 patients), most had an open fracture in their clinical history (46/89; 52%), followed by closed fractures (39/89; 44%), and finally, a small percentage had an oncological cause (4/89–4%).
The most frequently affected site was the forearm. Specifically, the radius was the most affected bone segment (64/156; 41%), followed by the ulna (49/156; 31%). The involvement of both the radius and ulna (21/156; 14%) was as common as the involvement of the humerus (22/156; 14%).
Size of the bone defect and type of spacerThe average size of the defect was 4.5 cm, with a range from 0 to 12.5 cm. Most (81/156; 52%) had a defect between 2 and 5 cm in size. Next in frequency were defects larger than 5 cm but less than 10 cm (57/156; 37%), defects smaller than 2 cm (13/156; 8%), and finally, defects larger than 10 cm (5/156; 3%).
Considering the location of the bone defect, the average defect size was 2.5 cm at the humeral level, while at the forearm level, the average size increased to 5 cm.
The choice of spacer material was PMMA in 100% of cases. The decision to add antibiotics to the cement was reported in 13 studies. Two studies reported adding antibiotics without specifying which, three studies used gentamicin, one study used vancomycin, one study used a combination of vancomycin and gentamicin, one study used either vancomycin or tobramycin, one study used a combination of vancomycin and tobramycin, one study used vancomycin and meropenem either independently or combined, and finally, in three studies, no antibiotics were added to the cement. Overall, antibiotics were added in 77% (105/136) of cases. The most commonly used antibiotic (either alone or combined) was vancomycin (54/125; 43%), followed by gentamicin (26/125; 21%).
Time interval and type of graftThe average time between spacer placement and its replacement with bone graft was 9.5 weeks. This parameter, reported in 13/15 studies, showed considerable variability from study to study, with average values ranging from 6 to 29 weeks.
The type of graft used was almost entirely autologous iliac crest graft (136/156; 87%), followed by RIA (17/156; 11%) and autologous non-vascularized fibula graft (3/156; 2%).
Bone union time and follow-upThe bone union time was reported in 11 studies. The global mean value was 5.5 months, but there was considerable variability from study to study (average range from 3.5 to 9 months).
When categorized based on the size of the bone defect, the mean time to union was 4.5 months for defects equal to or less than 2 cm, 6.5 months for defects between 2 and 5 cm, and 7 months for defects larger than 5 cm. These values were not significantly different (p = 0.112).
The mean follow-up duration, reported in nine studies, was 48 months. The difference between studies was considerable, with average follow-up values ranging from 24 to 102 months.
ComplicationsOverall, the complication rate was 21% (33/156), with a reported range from 0 to 75%. Two studies reported no complications.
The most frequent complication was infection (9/33–27%), which required one or more superficial debridement procedures in 5 cases, graft renewal in 1 case, and revision with non-vascularized fibula graft in 1 case; there was a failure to consolidate in 1 case and amputation of the limb after multiple salvage attempts in 1 case.
The need to revise the graft for non-septic causes occurred in 4 cases (12%). In 1 case, two additional iliac crest grafts with added demineralized bone matrix were necessary; in 1 case, an additional iliac crest graft was required following initial RIA; and the remaining 2 cases were managed with additional iliac crest grafts.
Aseptic failure of consolidation was described in 5 cases (15%). Of these, two were revised with a non-vascularized fibula graft after multiple attempts with additional grafts, resulting in consolidation in 1 of the 2 cases.
Overall, 6 cases (6/156–4%) did not achieve bone union.
Additional complications included adhesion formation or stiffness (7/33); the development of algodystrophy (1/33); seroma formation (1/33); the need for ulna shortening (2/33); irritation related to fixation devices, leading to their revision or removal (2/33); peripheral nerve paralysis (2/33); and peri-implant fracture (1/33).
When complications were divided based on anatomical site (4/22 (18%) at the humeral level and 29/134 (22%) at the forearm level), the difference was not statistically significant (p = 0.931).
留言 (0)