In our study, ST MRI resulted in 100% sensitivity and specificity in identifying a PP tear in both symptomatic and asymptomatic patients. The standard MRI examination without a ST has a sensitivity rate of 75% for a PP tear and 60% for MTP subluxation evaluation in symptomatic patients.
Among the non-invasive methods used in the diagnosis of PP disease, ultrasound and standard MRI currently play equally important roles. Various studies and systematic reviews [11, 16,17,18,19,20,21] on the greater diagnostic validity of one or the other technique, often with non-univocal results, are available in the literature. However, both methods have limitations in identifying all PP tears.
A recent study by Donegan et al. [16] compared the diagnostic accuracy of MRI and high-resolution dynamic ultrasonography in evaluating PP pathology, with surgical confirmation as the reference standard. The study included a multicentre retrospective analysis. The study's findings indicated that MRI had a sensitivity of 60%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 33%. The overall diagnostic accuracy of MRI, compared to intraoperative findings, was 66%. On the other hand, high-resolution dynamic ultrasonography showed a sensitivity of 100%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 100%. Compared to intraoperative findings, the overall diagnostic accuracy of ultrasonography was 100%. Although it was not statistically significant, high-resolution dynamic ultrasonography demonstrated greater accuracy than MRI in diagnosing PP pathology in the lesser MP joint.
Contrary to the current study's findings, a meta-analysis conducted by Duan et al. revealed different results [17]. The meta-analysis included studies that investigated the diagnostic detection of MRI or ultrasound for PP tears, with surgical criteria used as the reference test. A total of seven studies, comprising 246 PP tears, were included in the meta-analysis. The results of the meta-analysis indicated that MRI exhibited higher diagnostic accuracy than ultrasound for the detection of PP tears. The sensitivity, specificity, positive likelihood, and negative likelihood ratios for MRI were 95%, 54%, 2.08, and 0.08, respectively. In comparison, ultrasound had a sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio of 93%, 33%, 1.20, and 0.35, respectively. The summary receiver operating characteristic curve also indicated that MRI had superior diagnostic accuracy compared to ultrasound.
Albright et al. [18] conducted a systematic review and meta-analysis to assess the diagnostic accuracy of MRI and dynamic ultrasound for PP tears. The review included studies published in databases such as MEDLINE, CINAHL, and Clinicaltrials.gov until May 2020. MRI's pooled sensitivity and specificity for PP tears were 89% and 83%, respectively. Results showed that the sensitivity and specificity for ultrasound were 95% and 52%, respectively. Overall, MRI demonstrated superiority over ultrasound in diagnosing PP tears. However, ultrasound was more sensitive than MRI, suggesting that a negative ultrasound result would likely rule out a PP tear when there is uncertainty based on a physical examination alone.
In another comparative study, Klein et al. [11] examined the diagnostic performance of MRI and ultrasound in 51 patients with a suspected unilateral PP tear, specifically at the second metatarsophalangeal joint. All 51 patients were examined intraoperatively, and 46 PP tears were identified. The sensitivity, specificity, positive predictive value, and negative predictive value of MRI were 73.9%, 100%, 100%, and 29.4%, respectively. For ultrasound, the corresponding values were 91.5%, 25%, 91.5%, and 25%, respectively. Interestingly, MRI detected four collateral ligament tears that were not identified on ultrasound. Based on these results, both MRI and ultrasound are considered suitable modalities for imaging PP pathology.
A study conducted by Sung et al. [19] investigated the concordance between MRI findings and intraoperative results in a cohort of 41 patients (38 females and three males; 45 feet) with an average age of 52.1 years. Intraoperatively, 41 cases of PP tear and four cases of intact ligaments were identified. The assessment of accuracy, sensitivity, specificity, positive predictive value, and negative predictive value yielded values of 96%, 95%, 100%, 100%, and 67%, respectively. Moreover, the clinical diagnosis of PP injury achieved a high level of accuracy, with the condition correctly identified in 41 out of 45 patients (91%) within the study population.
Nery et al. [20], in their study, compared the evaluation of MTP plantar plates with arthroscopic findings in 35 patients. Using the standard examination, they observed a level of precision of 88.5% in senior radiologists and 77.0% in less experienced radiologists.
Yamadà et al. [21] investigated the diagnostic performance of direct and indirect MRI features for PP tears at II and III MTP, using surgical findings as the reference standard. The study encompassed a retrospective analysis of 23 patients who presented with symptomatic instability of lesser MTP joints and had previously undergone preoperative 1.5-T MRI and a subsequent surgical evaluation. A total of 45 lesser MTP joints were included in the analysis. The researchers found that the presence of pericapsular fibrosis exhibited high sensitivity (91.2%), specificity (90.9%), and accuracy (91.1%) for the diagnosis of PP tear. Furthermore, they determined that the PP–proximal phalanx distance yielded a sensitivity of 64.7%, specificity of 90.9%, and accuracy of 71.1% in diagnosing PP tears when a cutoff value of 0.275 cm was applied.
Even in MRI studies with higher levels of precision, an accuracy of 100% is never achieved. Our study aimed to evaluate whether a simple additional sequence could be a valid tool to achieve greater accuracy in diagnosing both PP tears and dysfunction.
Crucially, among non-invasive methods, forefoot MRI is not an operator-dependent investigation, and it provides more detail when compared with ultrasound, particularly on bone pathology. Compared to ultrasound, however, its current limitation is the inability to provide a dynamic evaluation simulating the normal load to which the MP joints are subjected.
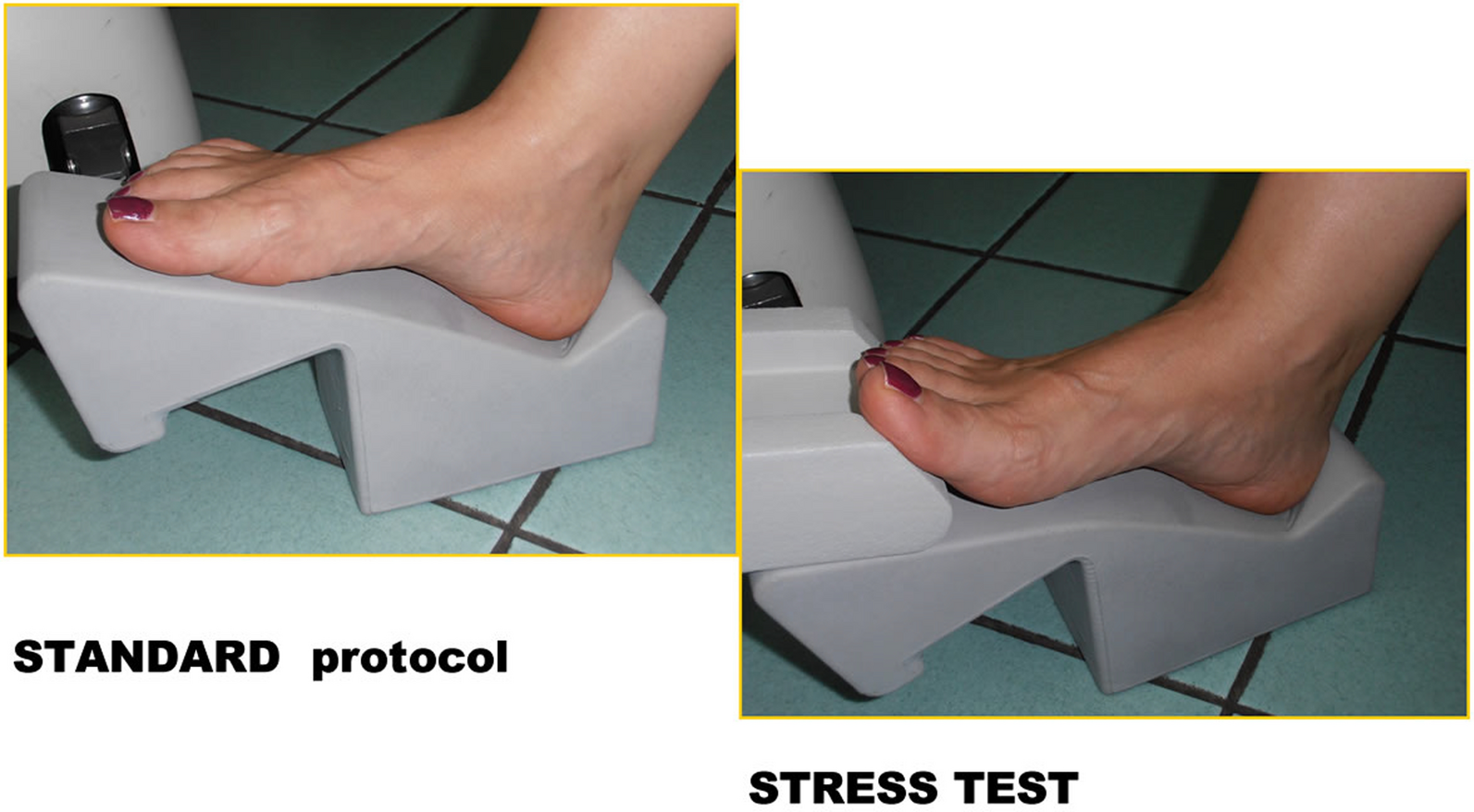
The ST appeared to significantly increase the diagnostic accuracy of MRI in evaluating PP disease compared to the standard examination in our study and to previously reported data from other studies. In our opinion, the ST should not always be performed, but it should be performed in cases where there is a clinical suspicion of a lesion or instability of the PP or when a small PP tear is noted during the standard examination or there is a doubt about it.
The ST is simple and quick to perform (since it is a single sagittal T2-weighted sequence lasting about 2.30 min) for both the operator and the patient. The ST is a sequence that should be added at the end of the examination as a complement, without replacing the sagittal T2-weighted sequence in the standard examination. It has the advantage of negligibly increasing the overall duration of the exam, and it led to an improvement in both sensitivity and specificity in diagnosing a PP tear or dorsal subluxations of the proximal phalanx in our study. Potential limitations include possible poor patient compliance due to discomfort in maintaining the position or potential motion artifacts. It is important to note, however, that none of these situations occurred in any patient within our study sample.
Among the invasive diagnostic procedures, arthrography is now practically no longer required in the diagnosis of a PP tear, while the use of arthro-MRI is limited to doubtful cases due to the cost of the examination, despite the fact that distension of the joint with contrast media (MdC) allows the lesion to be easily identified.
When compared with arthro-MRI [22] (after the intra-articular injection of MdC, which is invasive), standard MRI + ST is a non-invasive and less expensive investigation that is also feasible with dedicated equipment.
Dinoà et al. [23] explored the difference between identifying a PP tear without and with contrast-enhanced and fat-suppressed MRI. This study examined a total of 249 contrast-enhanced forefoot MRI scans obtained from patients diagnosed with metatarsalgia between June 2012 and June 2013. The scans were reviewed by two specialized radiologists with expertise in musculoskeletal imaging. Among the patients included in the study, 59 individuals were identified as having a PP tear; it is noteworthy that 59% of these were female. Most patients with a PP tear (81.4%) had a single tear in one of their MTP joints. However, a small number of patients (seven out of 59) had a PP tear in each foot, three out of 59 patients had two PP tears in one foot, and only one out of the 59 patients had three lesions in one foot. Pericapsular fibrosis was observed in 70.5% of the PP tears in pre-contrast sequences. However, for the remaining 29.5% of the lesions, the presence of the tear was only evident after administering a contrast agent containing gadolinium. This highlights the substantial proportion of PP tears that became visible on MRI scans only after the administration of gadolinium.
In this case, the use of contrast agents increased the diagnostic capacity of the examination. Yet, the cost and potential danger of using contrast agents and the contraindications for an MRI examination make it an undesirable option.
Our study therefore shows the potential to reach a diagnosis of a PP tear with the simple addition of the ST when using any type of MRI machine. Ours is a preliminary study with a limited sample; although the results are very promising, other similar studies that can confirm our results are required. Should other studies report similar values of high sensitivity and specificity in the diagnosis of a PP tear with the use of the ST, there would be many advantages in normal diagnostic practice, such as being able to confirm or reject a clinical suspicion of a PP tear.
Firstly, it could mean that any type of MRI machine could be used, so there would not be the need for high-magnetic-field machines, which are often a prerequisite in the case of arthro-MRI or MRI with contrast agents. An MRI study with a sectoral system would also allow us to reduce the not-inconsiderable percentage of claustrophobic patients.
Furthermore, the duration of the examination would not increase significantly, making the examination easily reproducible.
MRI reveals information that cannot be obtained with ultrasound, allowing, first and foremost, the study of any concomitant bone pathology (e.g. bone marrow oedema). However, ultrasound can allow more reliable dynamic tests in real time. With the ST, which places a similar tension on the joint to that which can be achieved with ultrasound, previously unrecognized lesions can be identified.
Currently, there is no other article in the literature that evaluates the diagnostic accuracy of the ST, so further investigations are necessary. The main limitations of our study are the small number of patients and the recruitment of positive cases (referred by orthopaedic colleagues with a specific clinical question: to evaluate a PP tear). This situation is not easily reproducible in routine clinical practice, where it is often difficult to formulate a specific clinical question due to the frequent coexistence of multiple findings (such as a PP tear, arthritis, and tenosynovitis), which can complicate the primary diagnostic hypothesis.
In the case of a PP tear, significant improvements in symptoms are achieved after surgical treatment.
Baker et al. [24] performed a systematic review and meta-analysis of PP repairs; a total of 12 studies with 537 PP tears were included in the analysis. It revealed a significant reduction in Visual Analog Scale (VAS) pain scores postoperatively, with a pooled mean change of − 5.24 (95% CI − 6.09 to − 4.39). These findings were consistent across all studies that reported VAS pain. Notably, the dorsal approach showed promising outcomes, displaying an improvement in both VAS pain scores and American Orthopaedic Foot and Ankle Society (AOFAS) scores, with relatively narrow 95% confidence intervals. The summary estimates generated for pain and function at the 1-year follow-up in patients undergoing direct dorsal repair further support the predictability and effectiveness of this approach.







留言 (0)