Hypertension is a major risk factor for cardiovascular diseases. Many studies have demonstrated that reducing dietary sodium (salt) intake and increasing potassium intake, found abundantly in fruits and vegetables, can effectively lower blood pressure [1, 2]. It would be ideal if people could consume the optimal intake of sodium and potassium to maintain good health. However, dietary habits are greatly influenced not only by physiological needs but also by external factors such as cultural food practices, climate, religion, and socioeconomic status (SES), which encompasses income, education, and occupation.
Previous research indicates that people with low SES are more likely to consume higher amounts of sodium and lower amounts of potassium, as well as fewer potassium-rich fruits and vegetables. This trend has been observed in both Western countries [3, 4] and East Asia [5, 6], where salt consumption is notably higher than in Western countries. The NIPPON DATA 2010 cohort [6], which included participants from the National Health and Nutrition Survey in Japan 2010, revealed that higher urinary sodium-to-potassium ratio and lower estimated 24-h urinary potassium excretion were observed among individuals with lower equivalent household expenditure (household expenditures divided by the square root of the number of family members) or educational attainment. These associations are attributed to the costs of fresh foods such as fruits and vegetables, which are rich in potassium, have low energy density, and may be less affordable for families with limited budgets. Additionally, individuals with higher educational levels are more likely to adopt health-promoting behaviors [7].
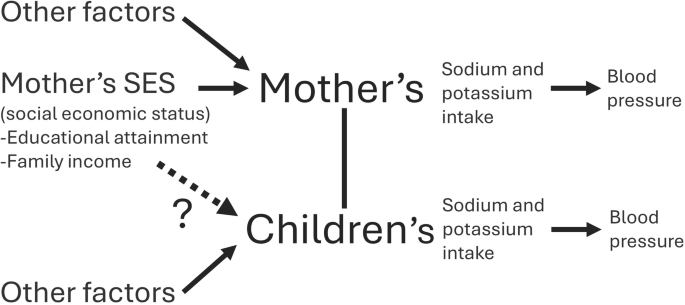
Ito et al. [8] investigated the association between estimated 24-h urinary sodium and potassium excretion as well as the sodium-to-potassium ratio and maternal SES in children aged 6–12 years (mean age 7.8 years) attending a public elementary school in Okinawa prefecture and their mothers (mean age 39.0 years). The study found an inverse relationship between the mothers’ estimated 24-h urinary sodium excretion and sodium-to-potassium ratio and household income, even after adjusting for age and body weight. These findings are consistent with previous reports [3,4,5,6]. Conversely, no significant association was observed between the mothers’ educational attainment and urinary mineral excretion (sodium, potassium, and sodium-potassium ratio) after adjusting for age and body weight. It is known that higher educational attainment often correlates with higher income [9] and this study [8] also found a significant positive correlation between maternal education and household income. Ito et al. [8] suggested that one reason for the lack of association between educational attainment and urinary sodium and potassium excretion might be due to the narrow range of educational levels among study participants.
On the other hand, among the children, no association was found between household income or maternal educational attainment and urinary mineral excretion (sodium, potassium, and sodium-potassium ratio) [8]. Since salt intake is positively associated with blood pressure in childhood as well as in adults [10], and childhood blood pressure is associated with blood pressure [11] and organ damage [12] in adulthood, optimal sodium and potassium intake during childhood is important for preventing future hypertension and cardiovascular diseases. In particular, children aged 6–12 years, the focus of this study, are more likely to eat at home and are influenced by family meals compared to older adolescents. Ito et al. [8] suggested that one reason why children were less affected by economic disparities in the family meals was their consumption of nutritionally balanced school lunches, which ensured appropriate sodium and potassium intake during weekday lunches.
In Japan, the School Lunch Program Act established in 1954, mandates the provision of nutritionally balanced school lunches, aligned with nutritional requirements for school meals. The benefits of these school lunches likely extend beyond merely improving sodium and potassium intake at the time, as children may be more receptive to healthier foods (e.g., fruits and vegetables) at home due to the formation of optimal eating habits that result from repeated exposure to school lunches [13]. Similarly, in the United States, the Healthy, Hunger-Free Kids Act of 2010 (HHFKA) [14] aims to provide all children with the nutrients required for healthy growth and development. Efforts are underway to provide nutritionally balanced school meals with gradual improvements in sodium and potassium intake planned over a 10-year period. One report evaluating the HHFKA found that children from low-income, low-middle-income, and middle-high-income families who participated in the National School Lunch Program reported superior diet quality, including high vegetable and fruit intake, compared to non-participants [15]. Given the anticipated widening of economic disparities in Japan, the findings of Ito et al. [8] represent an important first step in understanding strategies to prevent future cardiovascular diseases in children.
As Ito et al. [8] stated in their study’s limitations, the research focused on a public elementary school in Okinawa Prefecture, a region with a distinct climate and culture compared to other parts of Japan. Further studies across diverse regions of Japan are necessary to determine the generalizability of these findings and to enhance knowledge of hypertension prevention strategies for both parents and children.






留言 (0)