
記住我




We performed an ambidirectional cohort study involving 148 subjects consecutively recruited over a six-year period from an outpatient rehabilitation service at a tertiary care university hospital. The study aimed to explore the relationship between alterations in swallowing safety (penetration, aspiration, or residue) as identified by FEES and the incidence of pneumonia. Subjects with muscular or neurological involvement at risk of functional oropharyngeal dysphagia were included. The exposed cohort was constituted by those subjects with alterations in swallowing safety detected in FEES and the unexposed cohort included subjects without such alterations.
The exclusion criteria were subjects with mechanical dysphagia (tumors or anatomical abnormalities of the upper aero-digestive tract), active cancer, cancer chemotherapy, pregnancy, and asplenia.
Pneumonia was defined as the presence of the symptoms and signs of acute lower respiratory infection (cough, purulent sputum, fever, tachypnea, tachycardia, leukocytosis, or leukopenia), and the presence of infiltrates on a chest radiograph [28, 29].
Socioeconomic level in Colombia is classified according to the place of residence and the payment of public services. Low socioeconomic level is those classified as 1 and 2, medium socioeconomic level to levels 3 and 4, and high socioeconomic level to levels 5 and 6.
Evaluation of SwallowingAll subjects received a clinical evaluation of swallowing that included a search for signs and symptoms of oropharyngeal dysphagia and an assessment of head and neck muscle function. Further details of the clinical evaluation are included in the supplementary appendix. Subjects were considered at risk of oropharyngeal dysphagia when one or more of the following abnormalities were present: symptoms of pharyngeal dysphagia; any compromise of gag reflex; a gastrostomy, jejunostomy, or nasoenteral feeding tube; head or neck muscle compromise; or an orotracheal or tracheostomy tube for more than 14 days. When the clinical evaluation of swallowing was completely normal, a FEES was not performed. Subjects underwent a FEES in case of any abnormality in the clinical evaluation of swallowing or oropharyngeal muscle motor compromise.
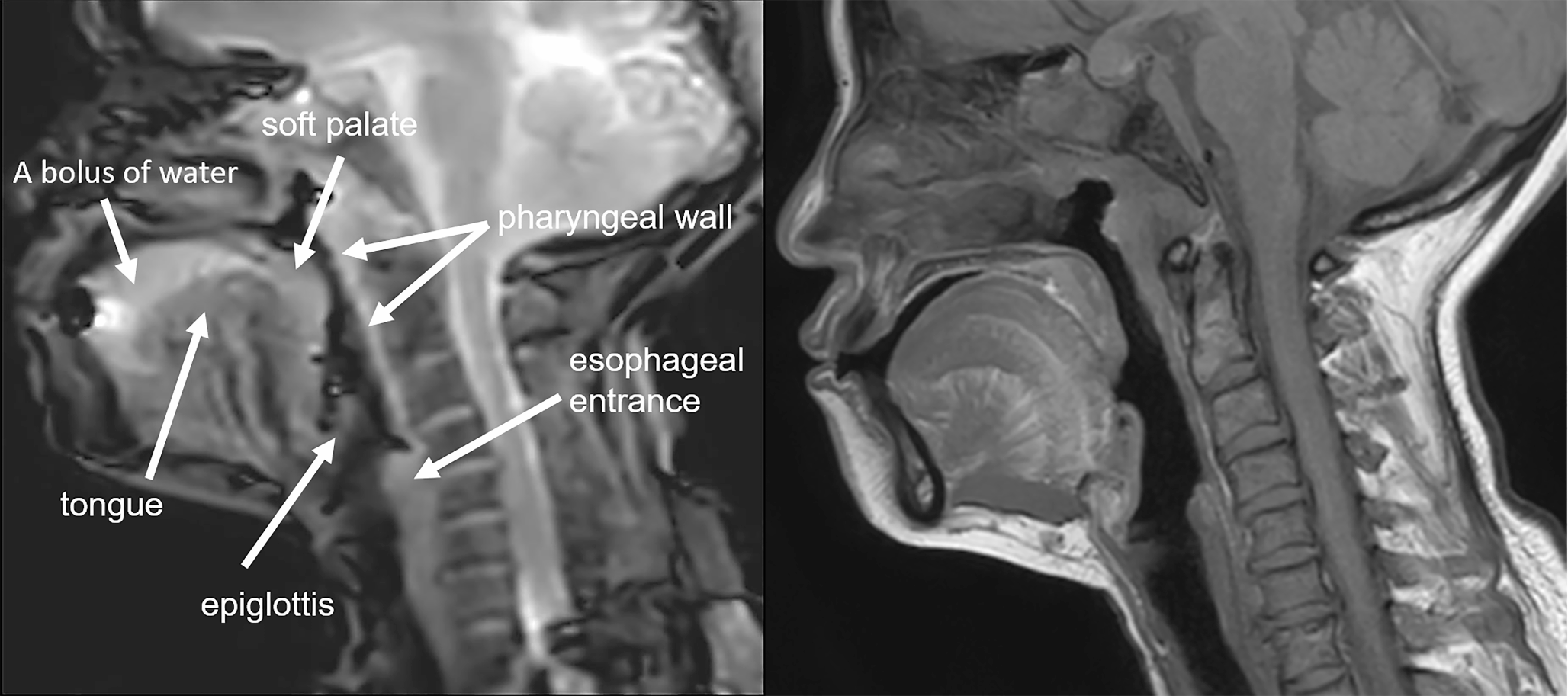
The FEES studies were conducted by a pulmonologist with more than 2 years’ experience and 50 completed FEES procedures along with a speech language pathologist. The studies were done with the subjects in a seated position, without anesthetics, and using a flexible fiberoptic endoscope with an outer diameter of 4.1 mm connected to a video system (Olympus LF-GP, Center Valley, PA, USA). The endoscope was lubricated with water-soluble gel, introduced through one of the nostrils, and advanced into the pharynx. The examination included an anatomical and functional exploration of the upper aero-digestive tract, including vocal cord motility. Subsequently, the tip of the endoscope was placed at the velopharynx. A first swallow without food was conducted to evaluate the pharyngeal contraction and the elevation of the larynx. The evaluation of swallowing continued by observing the bolus transport of green-colored foods of different consistencies from the back of the oral cavity to the esophagus and searching for any abnormality in deglutition.
The FEES unit, connected to the video equipment, recorded the procedures. These recordings were then reviewed in real-time and, when necessary, in slow motion after the examination. Further details of the FEES protocol can be found elsewhere [30].
An association with pneumonia was explored for the following alterations of swallowing safety as detected in FEES: residue, penetration, and aspiration. Residue consisted of the persistence of material in the pharynx (pharyngeal walls, valleculae, epiglottis, pyriform sinuses, and base of the tongue) after swallowing, penetration consisted of the entrance of material into the laryngeal vestibule, and aspiration consisted of the passage of material into the trachea below the vocal cords [30]. Given the existing literature validating the intra- and inter-rater reliability [14,15,16] and accuracy [17] of the FEES findings we investigated and our study’s focus on other aspects, such as the prognostic capacity of FEES for predicting the occurrence of pneumonia, we did not include measurements of intra- and inter-rater reliability in our study [14, 15].
Follow-upThe follow-up for the 148 patients spanned five years, comprising two phases. Phase I, the retrospective phase, occurred between the onset of dysphagia (e.g., stroke, brain trauma, or central nervous system infection causing dysphagia) and the FEES. For subjects with a completely normal clinical examination of swallowing, who did not require FEES, this time was between the event causing disability requiring referral to our rehabilitation program and the clinical examination of swallowing. These patients with normal swallowing were included in the unexposed cohort for comparison with the exposed cohort (patients having alterations in swallowing safety detected by FEES). We included this retrospective phase of follow-up in order to analyze the period in which subjects did not receive swallowing rehabilitation, because at the time dysphagia was diagnosed, the subjects were admitted to a standardized protocol aiming to prevent respiratory complications and rehabilitate the swallowing process, which could weak the relationship between dysphagia and pneumonia. Phase II of the follow-up (prospective phase) was between the FEES or the normal clinical examination of swallowing and the end of the study. We determined the frequency of pneumonia during both phases of follow-up. The mean follow-up duration for Phase I was 1.8 years, and for Phase II was 3.7 years, resulting in a total mean follow-up of 5.5 years. Subjects underwent follow-up FEES when indicated by changes in the clinical evaluation of swallowing.
Ethical ConsiderationsThe study was performed according to the international standards of the Helsinki Declaration and national regulations. It was approved by the local Institutional Review Board and all subjects provided informed consent to participate in the study.
Statistical AnalysisQualitative variables were summarized as frequencies and percentages, and quantitative variables were summarized as means ± standard deviation (SD) if normally distributed, or median and interquartile range (25th–75th percentile) if non-normally distributed. The number of pneumonia episodes were analyzed in terms of incidence density rate (IR), namely the number of pneumonia episodes over the sum of the person-time of the people at risk (number of cases/100 people-years).
We implemented strategies to reduce selection bias, to control observer bias, and to prevent information loss, all of which are detailed in the supplementary appendix.
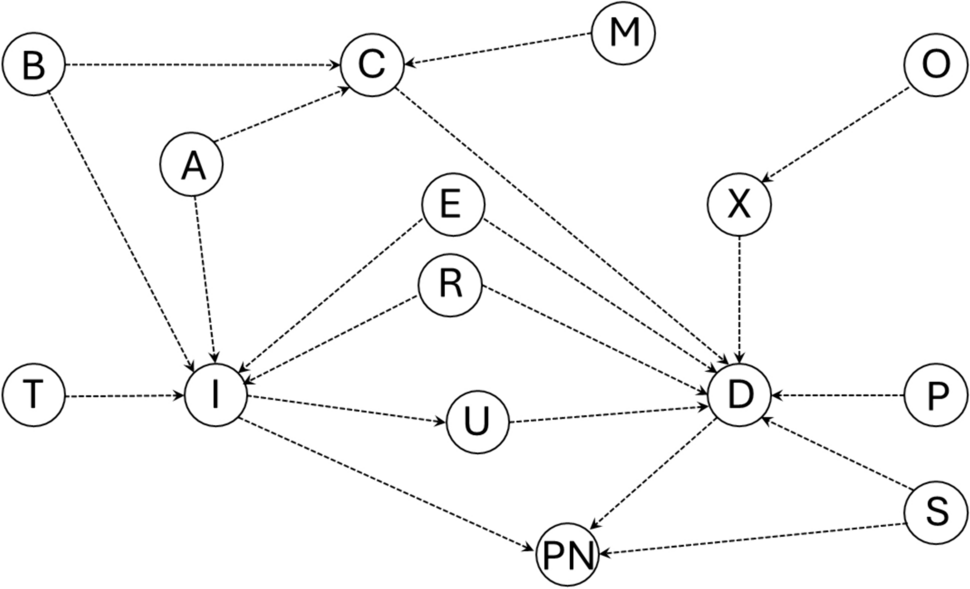
The independent variables included penetration, aspiration, and pharyngeal residue; the dependent variable was the number of episodes of pneumonia. To control confusion bias, we built multivariate logistic and negative binomial regression models that included the alterations of swallowing safety and the variables that could affect the association between dysphagia and pneumonia selected by biological plausibility and the drawing of directed acyclic graphs (DAG) (Fig. 1). The variables for the bivariate analysis selected by DAG were age at time of event, sex [31], smoking [32], chronic respiratory diseases (COPD, asthma, and other respiratory diseases) [33, 34], antacids [35], proton-pump inhibitors, oral hygiene frequency per day [36, 37], use of inhaled and systemic corticosteroids [38], diabetes, congestive heart failure, use of atypical and typical antipsychotics [39], high alcohol consumption defined as more than 3 drinks per day and/or more than 6 drinks per occasion in women or more than 8 drinks per occasion in men [40, 41], and immunosuppression [42]. The variables associated with the outcome (pneumonia) and the exposure (alterations of swallowing safety) in the univariate analysis with P < 0.25 at two tails and that fulfilled the criteria to be potential confounders according to DAGs (potential association with the exposure and outcome and not being intermediate variables in the causal path from the exposure to the outcome were entered into the multivariate model, and those with statistical significance in the multivariate model or those that changed the regression coefficient of the exposure under study by more than 10% were retained. Statistical significance was set at P < 0.05 (two-tailed).
Fig. 1
Causal pathways between comorbidities and pneumonia. Notes: A: age, sex, malnutrition, alcohol consumption; B: chronic obstructive pulmonary disease (COPD), asthma, diabetes; C: compromised pharyngeal function; D: dysphagia; E: antacids; I: immunosuppression; M: central nervous system depressant drugs, cerebrovascular disease, muscular and neuromuscular diseases, compromised state of consciousness, dementia, central nervous system cancer, head and neck cancer, degenerative neurological diseases; O: medications that decrease saliva production, hypertension; P: gastroesophageal reflux, esophageal dysmotility, upper gastrointestinal tract surgery, congestive heart failure; PN: pneumonia; R: inhaled corticosteroid, systemic corticosteroid; S: oral hygiene, smoking; T: cirrhosis; U: infections in the oropharynx and lacerations in the mouth, throat and esophagus; X: xerostomia
To investigate whether the association between penetration, residue, and the occurrence of pneumonia was independent or mediated by aspiration, we constructed a DAG illustrating the corresponding causal pathways (Fig. 2). Aspiration was the potential mediator variable, and thus, it was incorporated into the multivariate models of penetration and residue to assess whether the associations between penetration, residue, and pneumonia ceased.
Fig. 2
Causal pathway between alterations in the safety of swallowing detected in the FEES and pneumonia. Notes: R: pharyngeal residue; P: penetration; A: aspiration; PN: pneumonia
In our analysis of the effect of penetration, residue, and aspiration on pneumonia occurrence, we considered all subjects exhibiting the respective alteration, regardless of the presence of aspiration. For example, in the analysis of penetration, we incorporated subjects with both penetration and aspiration, as well as those with penetration alone.
Incorporating the aspiration variable into the multivariate models aimed to assess whether penetration or residue necessitated the presence of aspiration to increase the risk of pneumonia. This involved controlling for aspiration, effectively isolating the effect of penetration or residue (i.e., excluding the influence of aspiration) on pneumonia occurrence. If the association of penetration or residue with pneumonia occurrence were independent of the presence of aspiration, such an association would remain statistically significant even after introducing the aspiration variable into the corresponding models.
In our study, we analyzed aspiration, penetration, and pharyngeal residue as dichotomous variables. This approach allowed us to explore independent causal pathways in the multivariate analysis, which would have been challenging with ordinal scales. Moreover, incorporating ordinal, non-normally distributed variables into multivariable models presents statistical challenges that could interfere with achieving our main objectives.
The sample size calculation was performed with data from a prior retrospective study [43]. A total sample size of 148 subjects was calculated estimating a 20% annual incidence of pneumonia in the exposed cohort, a 4% annual incidence of pneumonia in the unexposed cohort, a 12% mean incidence (cohort exposed and unexposed combined), and a follow-up of 5 years (confidence level: 95%; power: 80%; including 10 predictor variables in the multivariate logistic regression model). The software used was Microsoft Excel 2007, and Stata SE, version 15.
留言 (0)