
記住我

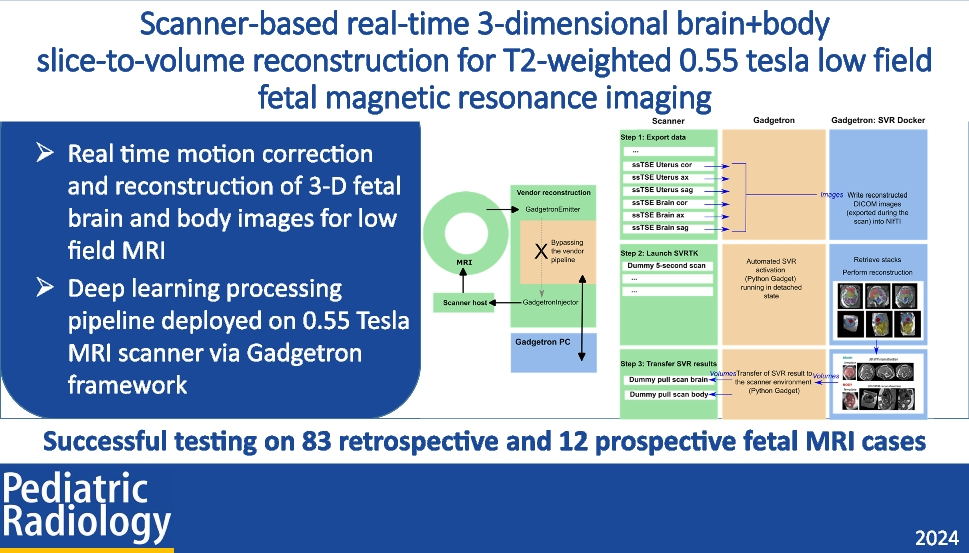
An overview of the proposed automated workflow implemented for a 0.55-T scanner is presented in Fig. 1. At first, the ssTSE images are exported to an external GPU-accelerated server (“Gadgetron server”) in real-time. Upon the collection of all ssTSE stacks, a 5-s dummy sequence is run for launching the SVR docker container (optimized for 0.55-T T2W contrast) on the Gadgetron server. Once the D/SVR results are available, 1-s dummy sequences are added to the exam card to pull the resulting T2W 3-D images to the MRI scanner and store them in PACS.
Fig. 1
Proposed pipeline for the integration of T2W 3-dimensional brain SVR and body DSVR reconstruction into scanner environment via Gadgetron. a Infrastructure setup. b Three-step process and flow of images and volumes between the scanner, during the acquisition of the single-shot turbo spin echo scans in coronal, axial, and sagittal orientations; the Gadgetron server; and the SVR container within the Gadgetron server. DICOM, digital imaging and communications in medicine; DSVR, deformable slice-to-volume reconstruction; MRI, magnetic resonance imaging; NIfTI, neuroimaging informatics technology initiative; PC, personal computer; ssTSE, single-shot turbo spin echo; SVR, slice-to-volume reconstruction; SVRTK, slice-to-volume reconstruction toolkit
Datasets, acquisitionThe fetal MRI data used in this study were acquired at St Thomas’ Hospital, London, as part of the ethically approved MEERKAT (REC: 21/LO/0742), MiBirth (REC: 23/LO/0685), and NANO (REC: 22/YH/0210) studies. All experiments were performed in accordance with relevant guidelines and regulations. Informed written consent was obtained from all participants.
The acquisitions were performed on a contemporary clinical 0.55-T scanner (MAGNETOM Free.Max, Siemens Healthcare, Erlangen, Germany) with a six-element flexible coil (BioMatrix Contour Coil, Siemens Healthcare, Erlangen, Germany) and a nine- element spine coil built into the patient table. The structural T2W stacks were acquired using a dedicated ssTSE sequence optimized for fetal imaging at 0.55 T (low field) [27] with TR = 1,460–2,500 ms, TE = 105–106 ms, 1.4-mm in-plane resolution, and 4.5-mm slice thickness. Each dataset includes 6–12 stacks covering the whole uterus, brain, and trunk regions using standard radiological orientations. The stacks were acquired in consecutive order without time gaps or changes in the maternal position.
The 0.55-T datasets used in this work were acquired between 2022 and 2024 and cover 20–40 weeks gestational age (GA) range (Fig. 2) including:
The deep learning training cohort: 384 stacks from 62 fetal datasets from 20–39 weeks GA range acquired during 05/2022–01/2023 period;
The retrospective evaluation (quantitative and qualitative) cohort: 83 fetal datasets from 22–39 weeks GA range acquired during 02/2023–08/2023 period;
The real-time testing cohort: 12 fetal datasets from 22–40 weeks GA range acquired during 01/2024–02/2024 period.
Fig. 2
Gestational age distributions of the 0.55-T T2W datasets used in this work for the training of the deep learning models, retrospective image quality evaluation, and real-time testing. GA, gestational age
The main selection criteria for the retrospective testing cases were singleton pregnancy, > 22 weeks GA, no significant structural fetal pathologies, good in-plane image contrast with high SNR, clear visibility of the whole fetus, and no breaks during ssTSE acquisition. This is a heterogeneous cohort with the maternal BMI varying between 22–43, different placental and fetal findings, and varying volume of amniotic fluid. Out of 88 originally inspected retrospective evaluation datasets, only four (5%) were excluded due to suboptimal image quality in the majority of stacks with severe in-plane signal loss caused by shading, extreme motion artifacts, or other acquisition-related factors. These cases were excluded because there was not enough image information (i.e., good-quality slices) for T2W 3-D SVR reconstructions. Furthermore, we did not include cases below 22 weeks due to the small size of the fetal organs compared to the intrinsic large slice spacing and low resolution in 0.55-T datasets that would be expected to compromise output reconstruction quality. This work focused only on cases without extreme structural anomalies since they represent the primary cohort of the available research 0.55-T scans at our institution.
Automated T2-weighted three-dimensional reconstructionThe proposed automated pipeline for combined T2W 3-D brain + body D/SVR reconstruction is summarized in Fig. 3. This is an extension of the previous work for automated T2W 3-D reconstruction of the fetal brain and thorax [15, 31] with both brain and body regions of interest (ROIs) trained on 0.55-T datasets using medical open network for artificial intelligence (MONAI) [32] network implementations. It includes global T2W 3-D localization of the brain and trunk in all stacks, followed by landmark-based reorientation to the standard radiological space, template selection, and classical rigid SVR and DSVR reconstruction. An additional reorientation step is applied to the final reconstructed images for refined alignment.
Fig. 3
Proposed automated combined T2W 3-dimensional brain SVR and body DSVR reconstruction pipeline for T2W 0.55-T fetal MRI including global T2W 3-D localization in motion-corrupted stacks (a), T2W 3-dimensional reorientation to the standard space (b), and average template creation and D/SVR reconstruction (c). 3-D, 3-dimensional; DSVR, deformable slice-to-volume reconstruction; SVR, slice-to-volume reconstruction; T2W, T2-weighted
Implementation of the global localization of the fetal head and body (Fig. 3) is based on a classical MONAI T2W 3-D UNet [33] segmentation network trained on 384 stacks from 62 0.55-T datasets with GA range 20–39 weeks with semi-manually created labels. Next, the reorientation of the brain and body ROIs to the same canonical space (Fig. 3) of all stacks is added in order to correct for large rotation and translation motion. It is implemented similarly to the previous works [15, 31] using MONAI T2W 3-D UNet of segmentation of four body (thorax, abdomen, heart, liver) and four brain (anterior brain, posterior brain, deep grey matter, cerebellum + brainstem) landmarks in ROI-cropped individual stacks. The networks were trained on 195 0.55-T cropped images with varying orientations and degrees of motion and semi-manual labels. The segmented landmarks are used for reorientation to the standard radiological space using classical point-based registration. After localization and reorientation, the processed stacks of slices are passed to the stack-selection [15] SVRTK function for generation of the average template space and mask and rejection of low-quality motion-corrupted stacks.
The final selected stacks are used in the rigid SVR [8] and rigid + deformable DSVR [9] functions for T2W 3-D brain and body reconstructions (Fig. 3) that were optimized to 0.55-T datasets with additional structure-based outlier rejection. Taking into account the native stack resolution (1.2 × 1.2 × 4.5 mm), the output resolution for T2W 3-D reconstructed images was selected as 1.0 mm.
Implementation and evaluation detailsAll pipeline components (deep learning and C + + reconstruction) are combined into one bash script. The code for the proposed brain and body reconstruction pipeline is publicly available at auto-proc-svrtk GitHub repository.Footnote 3 The proposed 0.55-T T2W 3-D D/SVR reconstruction pipeline is publicly available as a standalone Docker application at SVRTK Docker repositoryFootnote 4 that includes all required software installations as well as the network weights. The Docker is based on only central processing unit (CPU) processing and is executed on the CPU for straightforward deployment purposes. The recommended minimum Docker settings are > 20 gigabyte random-access memory and > height CPUs.
The evaluation of the proposed D/SVR pipeline is based on a set of retrospective datasets. The quantitative evaluation on 30 datasets is based on the localization distance and reorientation rotation errors and label Dice. The qualitative evaluation on 83 datasets is based on the grading of T2W 3-D reconstructed brain and body images in terms of image quality and visibility of organs by researchers with extensive experience in fetal MRI. The quality scores for the output T2W 3-D D/SVR images are as follows: 1—failed; 2—poor, 3—acceptable, 4—good (similar to the grading scheme in [5]). The evaluation was performed by three researchers with extensive experience in fetal and neonatal MRI (neuroradiologist: AL (2 years), clinical researcher: MH (> 5 years), technical researcher: AU (> 5 years)).
In addition, we run a supplementary comparison experiment to state-of-the-art reconstruction method based on implicit neural representation for slice-to-volume reconstruction (NeSVOR) [17] on five cases from 22 to 38 weeks GA range in order to demonstrate general performance in terms of reconstruction quality and time.
Gadgetron-based scanner deployment of three-dimensional reconstruction pipelineThe entire online pipeline was implemented using Gadgetron. As described above in Fig. 3 step 1, the reconstructed stacks are exported to the dedicated GPU-equipped Gadgetron server immediately after acquisition, and D/SVR reconstruction is subsequently performed, triggered by a 5-s dummy sequence. The total reconstruction time is approximately 6:42 ± 3:13 min, and the results are available immediately on the scanner console.
After all ssTSE stacks are acquired, a 5-s “launch” sequence is run as part of the protocol (Fig. 3 step 2). This establishes a connection between the scanner and the server and launches the SVR Docker container on the server as a detached subprocess, allowing the acquisition and reconstruction of the subsequent sequences in the exam card. The acquired data from the launch sequence is discarded. The final reconstructions for the body and brain are saved in the Gadgetron server.
As a last step to bring the D/SVR reconstruction to the scanner host in a controlled manner, two 1-s “pull” sequences are run towards the end of the protocol. A modified, highly accelerated magnetization-prepared rapid gradient echo sequence is employed for this purpose with the matrix size matched to the expected reconstruction. All brain reconstructions are resampled to an image matrix of 128 × 128 × 128 (128 slices) and the body reconstructions to 256 × 256 × 256 (256 slices) prior to this step. Resampling ensures consistent dimensions for reconstructed volumes, preserving the field-of-view across sequences without compromising result quality (e.g., cropped structures or missing slices). Similar to the sequence used to launch the SVR processing, these sequences are designed to establish the connection to the external server. The acquired data is then overwritten with the T2W 3-D SVR volume matrices, injected into the vendor image reconstruction chain, accessed by the scanner host, and subsequently exported to PACS.
Implementation detailsThe Gadgetron framework was installed on the dedicated external server and connected to the internal network of the MRI scanner. The sequences were modified to include the Gadgetron emitter and injector functors, enabling raw data to be sent to the external server for processing and the processed image data to be re-integrated into the scanner reconstruction pipeline. For each of the three tasks presented in this work, a pair of configuration files was created and the configuration file stored in the scanner host, defined by the sequence, points to the reconstruction and processing configuration file that is stored in the external server. The latter assembles the reconstruction and processing Gadgets the data streams through, including the Python-scripted external-language interface Gadgets that were developed for each task.
The code for the proposed Gadgetron-based D/SVR scanner integration for 0.55-T fetal MRI is publicly available at gadgetron-svrtk-integration GitHub repository.Footnote 5
留言 (0)