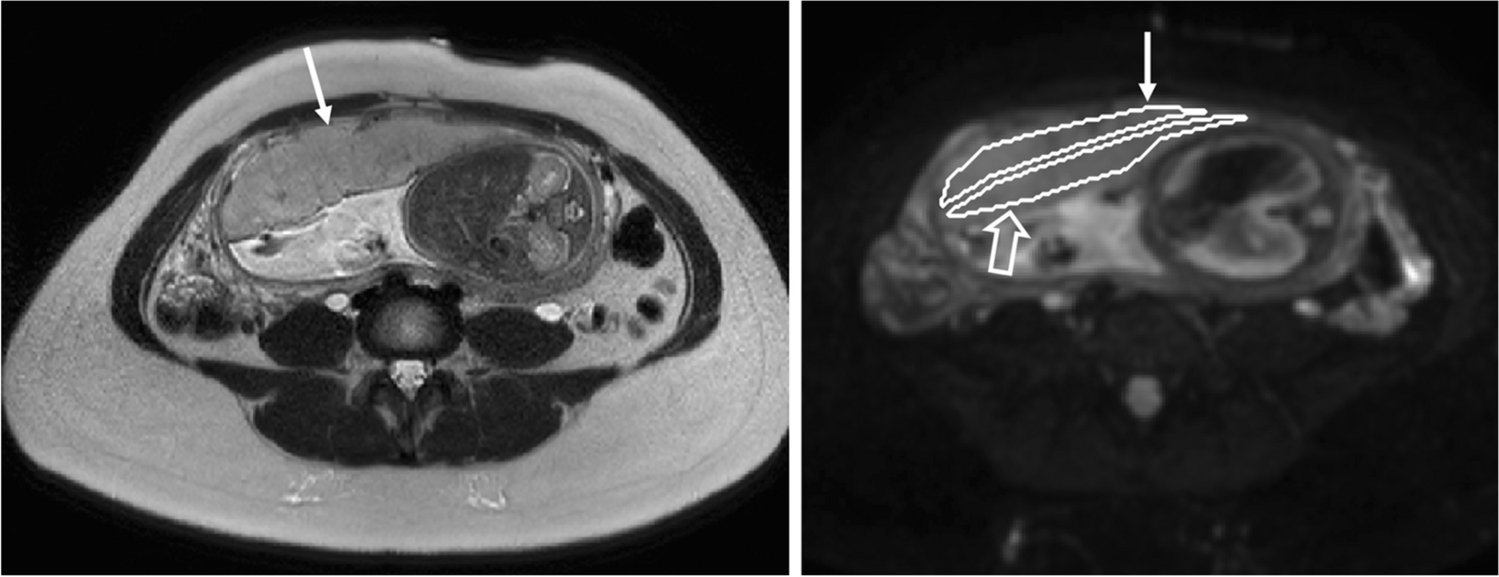
Only a few cases of metanephric stromal tumors have been described in the literature, which have mainly been diagnosed using CT as a preoperative diagnostic procedure followed by subsequent nephrectomy (see [5] for example). The starting point for diagnosis is usually – as in the case reported here – the ultrasound (US) examination, in which metanephric stromal tumor presents heterogeneously with solid and cystic parts, which can be isoechogenic, hypoechogenic, or hyperechogenic compared to the renal parenchyma [5]. On CT, a metanephric stromal tumor characteristically presents as a well-defined hypodense lesion, which shows varying proportions of cystic and solid structures. Strong contrast enhancement occurs in the urographic phase (see also [3]). Focal calcifications are also described, which may be helpful in the differentiation from nephroblastoma, which only rarely calcifies [2, 6]. In pediatric radiology, however, abdominal cross-sectional imaging is primarily performed using MRI for reasons of radiation protection. The characteristics of MRI diagnosis of pediatric metanephric stromal tumors have been little discussed in the literature to date. Kacar et al. describe a pediatric case in which the tumor appeared T1W hypointense and with a T2W hyperintense central cystic portion on MRI [6]. This description is similar to the case presented here. In contrast, Fan et al. describe the case of an adult patient whose lesion showed a T1W isointense signal and a T2W hypointense signal on MRI [5]. However, in view of the few case descriptions, it cannot be reliably postulated that the presentation varies according to age.
At present, it does not appear possible to make a reliable diagnosis of metanephric stromal tumor using radiological methods. However, radiology can play a decisive role in determining whether a tumor biopsy should be performed for further diagnosis, especially since nephroblastoma is the much more common diagnosis and does not require a biopsy before treatment. Jackson et al. have developed criteria to facilitate decision-making for or against performing a biopsy [8]. A biopsy is recommended if the tumor is of uncertain renal origin, a patient age >10 years, a tumor volume <200 ml at an age of 7–10 years or if it shows an atypical metastatic pattern [8]. In the presented case, the documented constancy in size of the tumor over several weeks cast doubt on the suspected diagnosis of nephroblastoma, which typically progresses rapidly. In addition to the criteria compiled by Jackson et al., the simultaneous presence of a constant lesion size, the absence of diffusion restriction, and the presence of multiple cysts were added by this case report as a combination that can be used to decide for a biopsy in the tumor board.
In summary, the diagnosis of rare pediatric renal tumors is known to be difficult based on radiological imaging alone. The low incidence of metanephric stromal tumors precludes any diagnostic routine from the outset, so that it seems advisable to make full use of the diagnostic spectrum, especially MRI.
If a renal mass is identified that cumulatively shows a small initial tumor volume, no size progression, no significant diffusion restriction, and multiple internal cysts, a tumor biopsy should be considered in order to rule out differential diagnoses of nephroblastoma. This can be of considerable consequence for patients, as nephroblastomas are usually treated without prior histologic confirmation by means of neoadjuvant chemotherapy and nephrectomy. Due to the characteristic hypovascularization of metanephric stromal tumors, CEUS is suitable for providing the surgeon with valuable information for the intraoperative determination of tumor margins in the context of kidney-preserving surgery and complete resection.
Consequently, the correct diagnosis can spare patients unnecessary chemotherapy and total nephrectomy.


留言 (0)