This study investigated the prevalence of psychotropic polypharmacy in Australians living with dementia whose caregivers sought external NPS support. It compared their demographics and NPS characteristics based on the presence of psychotropic polypharmacy. Psychotropic polypharmacy was found to occur in approximately half of the study cohort. Aside from a slight difference in age between the two groups, with the prescribed group being approximately 2 years younger than the non-prescribed group, we did not identify any other differences between those prescribed psychotropic polypharmacy and those who were not prescribed it, in demographics or NPS.
4.1 Prevalence of Psychotropic Polypharmacy
The prevalence of psychotropic polypharmacy in this study is relatively high compared with other studies involving people living with dementia in RACHs. In our study, 50.8% of referrals were prescribed psychotropic polypharmacy. In comparison, in a meta-analysis of studies pooling over 92,000 RACH residents with dementia in 12 countries, including Australia, Jester et al. [11] reported that 33% of residents were prescribed psychotropic polypharmacy. However, our study involved individuals specifically referred to a specialist service for NPS support, whereas the cohort in Jester et al. was not selected on the basis of their experience of NPS. Hence, it is likely that the prevalence of more severe NPS was greater in our study, and hence the proportion of people with NPS who were prescribed psychotropic polypharmacy was comparatively higher. Tan et al. reported on the medications used by patients admitted to a hospital-based cognitive assessment and management unit for moderate to severe NPS, delirium or other related neurocognitive disorders [31]. In that study, 96% of patients were prescribed an antipsychotic, 90% a benzodiazepine and 60% were on antidepressants, so the proportion of prescribed psychotropic polypharmacy would have been higher than in our study. These differences with our study may be attributed to the sample characteristics (e.g., sample size, demographic and clinical profile of participants, definition of psychotropic polypharmacy, care setting). As our study involved individuals with NPS from a unique setting (people seeking external, specific and targeted support for their NPS), it is plausible that the proportion of psychotropic polypharmacy would be lower than that reported by Tan et al. Further, a large 2021 cross-sectional study (n = 1,159,968) by Maust et al. found that 13.9% of community-dwelling older adults with dementia in the USA had been prescribed central nervous system-active or psychotropic polypharmacy medications [14]. The authors in that study defined psychotropic polypharmacy as concurrent exposure to three or more medications classified as antidepressants, antipsychotics, antiepileptics, benzodiazepines, nonbenzodiazepine benzodiazepine receptor agonist hypnotics and opioids and used for longer than 30 days consecutively. Given the more stringent definition of psychotropic polypharmacy and probable lower acuity of the participants in that study, it is understandable that the prevalence of psychotropic polypharmacy was lower than that reported in our study.
Thus, our numerical definition of psychotropic polypharmacy (co-prescription of two or more agents) may have augmented the prevalence rate of this concept, and it would have been much lower in our study if we had used a different numerical definition and calculation method. For example, the 2019 and 2023 American Geriatric Society (AGS) updated Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults define psychotropic polypharmacy as combinations of three or more central nervous system-active agents [15, 32]. However, we took a more conservative approach than the Beers Criteria® definition, as our cohort (people living with dementia) generally experiences high rates of medical comorbidities and is often prescribed multiple medications and thereby are more prone to adverse effects and drug–drug interactions; our sample was on average older than previous studies and specifically sought psychosocial support for their NPS. This approach is in line with the prescribing optimisation (i.e., reduction of over-prescription) of psychotropic drugs recommended by the International Psychogeriatric Association (IPA) guidelines for managing NPS [33]. The IPA has further elaborated on this by stating that the high rates of regularly used psychotropic drugs, especially antipsychotics, are suggestive of non-adherence to international clinical guidelines [33].
National peak bodies and public enquires in Australia have warned against psychotropic over-medication and the inappropriate use of psychotropics in older adults with dementia. For instance, the Royal Commission into Aged Care Quality and Safety identified the frequent overuse of psychotropics and recommended minimising or avoiding these medications in this population [34]. In response, a joint statement was issued in 2022 by the Australian Commission on Safety and Quality in Health Care, the Royal Commission into Aged Care Quality and Safety, and the National Disability Insurance Scheme Quality and Safeguards Commission [35]. This statement aims to address the overuse of psychotropics as chemical restraints, which are considered a form of restrictive practice and indicative of poor quality of care. More recently, the Australian Commission on Safety and Quality in Health Care released the Psychotropic Medicines in Cognitive Disability or Impairment Clinical Care Standard, endorsed by 25 key professional associations and consumer organisations, to guide clinicians, healthcare services and consumers on the safe and appropriate use of psychotropic medicines in people with cognitive disability or impairment [36].
4.2 Association Between Psychotropic Polypharmacy and other factors
In contrast to previous studies, we did not find any relationship between psychotropic polypharmacy and any of the variables tested, including age, sex, dementia subtype and NPI severity. A possible explanation for this could be the differing characteristics of studies, such as sample size, demographics and prevalence of NPS. In a population-based study performed in Denmark, Nørgaard et al. identified that age < 75 years, female sex, nursing home residency, polypharmacy (≥ 5 drugs) and prior psychiatric diagnosis predicted psychotropic polypharmacy [17]. Conversely, the meta-analysis by Jester et al. identified that psychotropic polypharmacy was slightly higher in males compared with females (odds ratio, 1.02) in univariate analysis, although this association was not present in the final multivariate analysis. In contrast to our study, neither of those studies assessed dementia subtype or symptoms. Hence, our study provides evidence that psychotropic polypharmacy is not associated with these variables in Australians living with dementia whose caregivers sought external behaviour support.
4.3 Strengths and Limitations
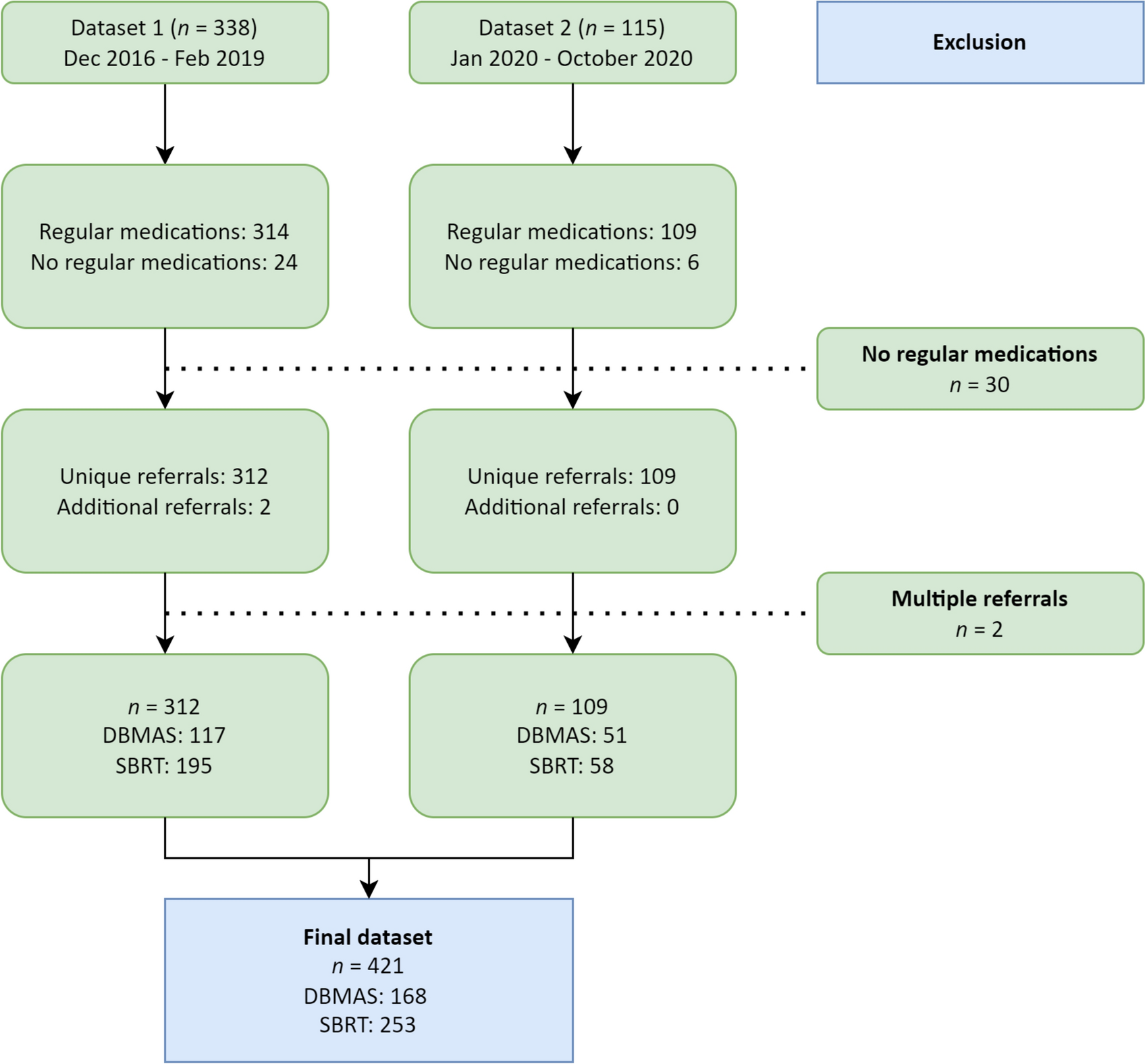
This study was of a retrospective, descriptive and observational design that applied a cross-sectional analysis. Hence, the general limitations of observational studies such as the lack of causation apply. Furthermore, there were additional limitations resulting from the data available for the study (e.g., other medications, dementia severity, medical comorbidities) that may have influenced its results. As comprehensive histories of medical diagnoses were not available for the referrals, it was not possible to determine the indication or the length of exposure for the psychotropic medications used. Although this prevented any assessment of whether the psychotropic co-prescribing was potentially appropriate or otherwise, such analysis was beyond the scope of this study. Further, our study did not consider ‘as needed’ (PRN) psychotropic medications, which may further augment the prevalence of psychotropic polypharmacy. Compared with previous studies, our sample size was relatively small. The ascertainment of dementia diagnosis may be lacking for some referrals in which dementia is suspected or reported by the caregiver (referrer). This may have resulted in overestimation of some of the findings. Another limitation is that we relied on two combined datasets from two separate quality improvement initiatives. Therefore, our analyses were estimated on a non-random subset of referrals. Thus, our findings might not necessarily be representative of all referrals. Further, merging the datasets in this study may have had an inflating or deflating effect on the overall prevalence rate of psychotropic polypharmacy because of the variability in the individual contribution of each dataset towards calculating this prevalence. Specifically, the two datasets spanned the pre- and post-COVID pandemic periods, which may have contributed to the higher prevalence rate of psychotropics in our study. These data periods also create an opportunity of comparison between pre- and post-pandemic trends and perhaps even demonstrate the rising trend in psychotropic drug use during the pandemic as outlined in previous studies [37]. However, this trend comparison is beyond the objectives of our study, and our study design and sample are limited in terms of characteristics (e.g., nature, size) and the timeline representativeness of these periods to answer this research question. Trend data of psychotropic polypharmacy of these periods with additional considerations (e.g., danger to self/others) should be investigated in future research. Additional limitations resulted from the fact that only 83% of referrals received an intake NPI assessment. This was largely owing to situations where the DSA consultant deemed it inappropriate or not feasible to perform the assessment at the initial consultation or point of contact. Examples of these situations include a lack of essential data available for the consultant to answer certain NPI questions, and/or the absence of a responsible caregiver who can provide these data at the time of NPI assessment. The lack of establishing a relationship between NPS and psychotropic polypharmacy in our study may not negate its existence. This was perhaps owing to setting-specific reasons, particularly the homogeneity of our sample, which was characterised by the presence of higher severity NPS than other RACH and community samples previously reported in the literature. Furthermore, given that nearly the entire sample was drawn from Australian RACHs, the findings of this study may not be applicable to other care settings (e.g., hospital, community), and the applicability of our findings may not extend beyond Australia. The findings specifically apply to aged care residents who are regularly using psychotropic medications and seeking specialised dementia support for NPS that affect their quality of life or that of their caregivers.
Despite these limitations, our study has several significant strengths. To our knowledge, this is the first study that assessed the relationship between psychotropic polypharmacy and NPS in Australians living with dementia whose caregivers sought external NPS support. The sample was drawn from across Australia and hence is likely to be nationally-representative. While the data were collated and analysed retrospectively, they were collected via DSA consultants and staff independent of this study (thus, they were blind to the objectives and design of the study), minimising the Hawthorne effect.









留言 (0)