Chronic progressive pulmonary aspergillosis within the irradiated field after stereotactic body radiotherapy: two case reports
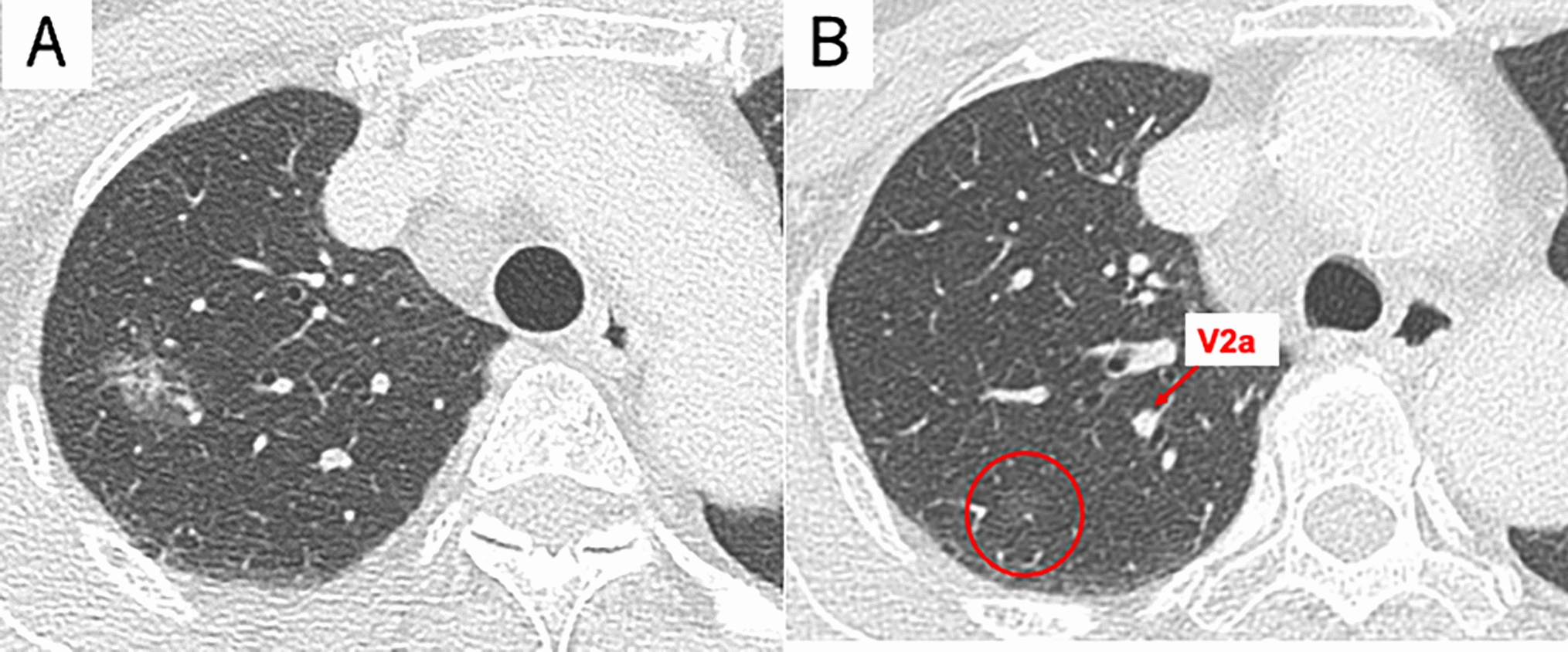
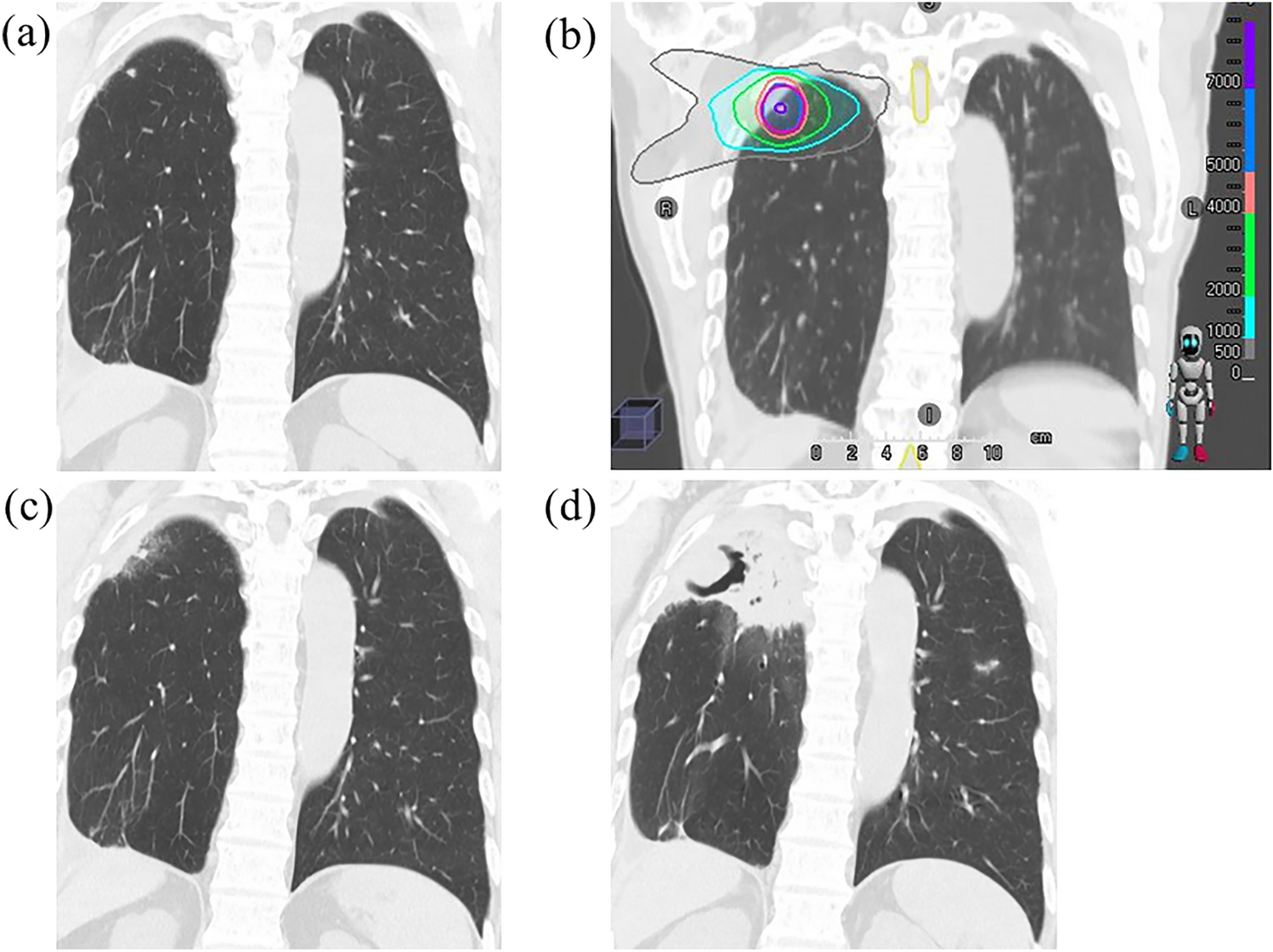
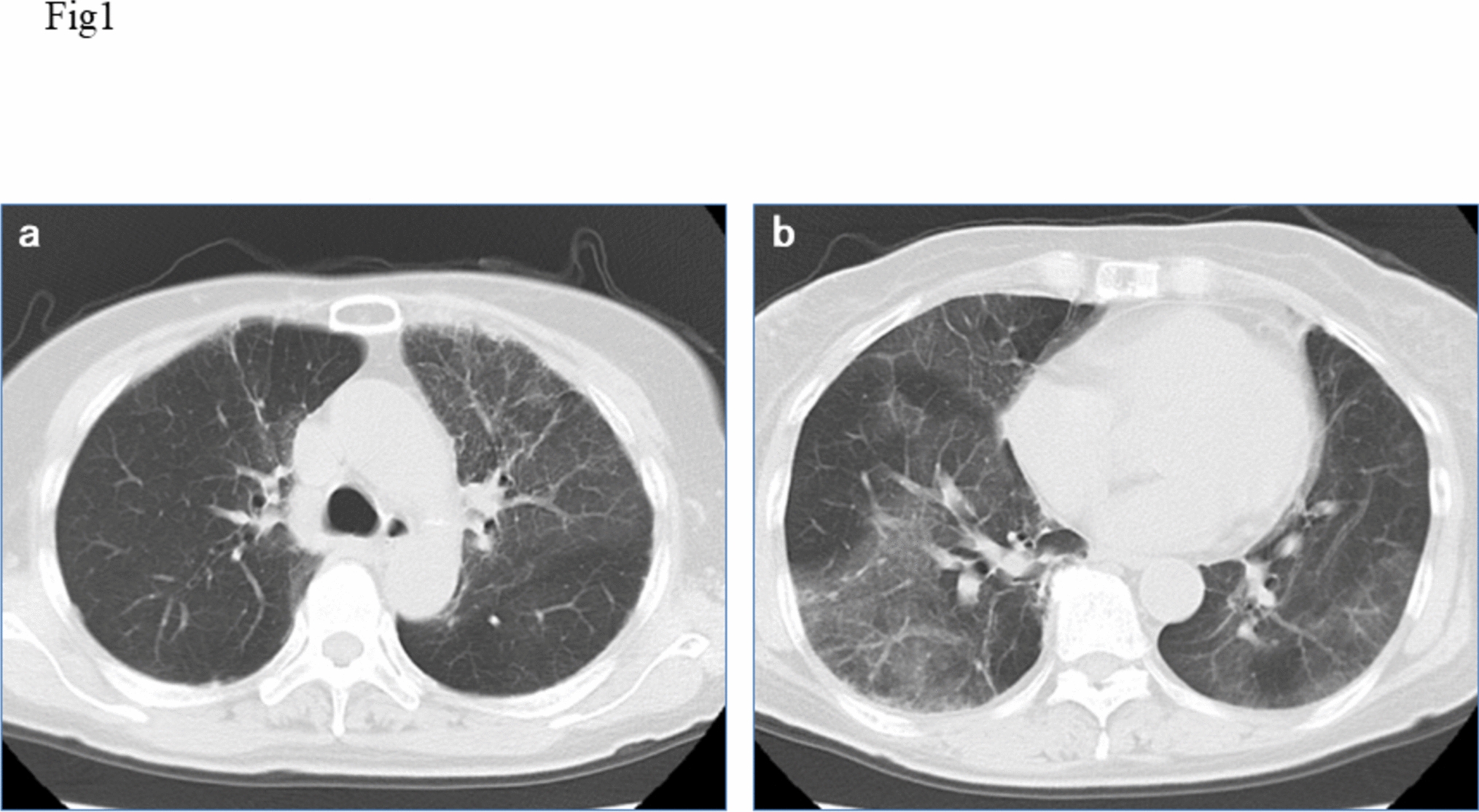
Stereotactic body radiation therapy (SBRT) is the standard treatment for patients who are medically inoperable or who refuse surgery with stage I non-small cell lung cancer (NSCLC). While acute lymphopenia following SBRT is documented, the long-term effects on the immune system and infectious disease remain unclear. In this report, we present two cases of chronic progressive pulmonary aspergillosis (CPPA) occurring within the irradiated field following SBRT for inoperable stage I NSCLC. Case 1 was a man in his 70 s with a history of smoking and a previous pulmonary resection and SBRT for metachronous primary lung cancer. He received SBRT for T1aN0M0 NSCLC in the right lower lobe as his third primary lung cancer. After 20 months, the patient developed a cough and sputum, and a computed tomography (CT) scan revealed a cavity shadow in the irradiated field, which led to the diagnosis of CPPA. Intravenous voriconazole was immediately started, and after 3 week’s administration, the symptoms improved, and the cavity disappeared. After 34 months, the patient died with no recurrence of CPPA and lung cancer. Case 2 was a man in his 80 s with a history of smoking and previous pulmonary resection for lung cancer. He received SBRT for T1cN0M0 NSCLC in the right lower lobe as his second primary lung cancer. After 19 months, the patient developed a fever, and a CT scan revealed a cavity shadow in the irradiated field, which led to the diagnosis of CPPA. Oral itraconazole was administered, followed by diarrhea and anorexia. After 22 days, the patient died. During the follow-up period, there was no recurrence of lung cancer. Risk factors for CPPA include a history of smoking and lung resection, common among candidates for pulmonary SBRT. When a cavity shadow develops following SBRT, differentiating consolidation as radiation pneumonitis, local recurrence, or infection can be challenging. When a cavity is identified on a follow-up CT scan after SBRT, it is crucial to include CPPA in the differential diagnosis.






留言 (0)