This study evaluated the predictive accuracy of six toric IOL calculators for eyes undergoing cataract surgery with toric IOL implantation, including both predicted and measured PCA. This finding underscores the necessity for comprehensive evaluations of these calculators to optimize postoperative refractive outcomes. Our findings indicate that the six calculators showed similar efficacy in predicting postoperative refractive astigmatism, with no statistically significant differences in mean APE or centroid of PE.
The mean APE across all calculators ranged from 0.56 D ± 0.37 (Barrett TK) to 0.63 D ± 0.46 (Barrett PPCA). These findings align with earlier research indicating mean APEs between 0.3 and 0.7 D for different toric IOL calculators [12, 17, 18]. The lack of statistically significant differences among the majority of calculators suggests that recent advancements in toric IOL calculation methods have potentially led to a convergence in predictive accuracy to some extent, which confirmed some results of previous studies [3, 18,19,20]. The proportion of eyes achieving an APE within clinically acceptable ranges varied among calculators. The Barrett MPCA calculator achieved the highest proportion of eyes with APE ≤ 0.50 D (56.6%), aligning with previous studies reporting similar proportions of 53.2% [21], 57.0% [22], and 65.6% [12].
Achieving the ideal refractive outcome with a single calculator has long been a pursuit in modern cataract surgery [23]. Kane and Connell indicated a significantly lower mean APE of Kane formula than other toric calculators [12], which is lower than our study. This could be due to their primary analysis relying on postoperative keratometry measurements, which eliminates the need to estimate the SIA. Our analysis aimed to determine clinical outcomes for each formula using preoperative keratometry values instead of postoperative parameters. This approach, referred to as “real-world analysis” in previous studies [12], aligns more closely with the practical needs of clinicians. While using postoperative parameters could theoretically eliminate the influence of SIA, clinicians are primarily concerned with the reliability of IOL calculations based on preoperative data. To minimize variability and the impact of SIA, our study incorporated several key methodological strengths: we included only cataract surgeries performed by a single, experienced surgeon; utilized a single type of intraocular lens; and applied a uniform, predetermined SIA value across all calculations. This design enhances the clinical relevance of our findings and offers a controlled environment for comparing the predictive accuracy of various toric IOL calculators under conditions similar to routine clinical practice.
Our analysis identified a statistically significant difference in mean APE between the Barrett PPCA and Barrett TK calculators (P = 0.02). This finding suggests a potential advantage in predictive accuracy for the Barrett TK calculator, which incorporates total keratometry measurements. Consistent with the previous study [18], when comparing the Barrett MPCA calculator to the Barrett TK, no significant difference was observed, despite the using of measured posterior corneal astigmatism data. Previous researches indicated that incorporation of TK values from IOL Master into Barrett toric calculations did not significantly enhance calculation accuracy [11, 20]. Historically, total corneal astigmatism was calculated based solely on anterior corneal astigmatism measurements, assuming a constant ratio between anterior and posterior corneal curvature. This approach has been associated with considerable prediction errors, including mean absolute errors (MAE) of up to 0.8 D ± 0.4 and centroid errors of 0.56 D at 180 degrees [24]. Mounting evidence indicates that incorporating PCA into toric IOL calculations can minimize postoperative refractive errors [10, 25, 26]. This nuanced result highlights the complex interplay between different approaches to corneal power assessment in toric IOL calculations. This finding underscores the potential benefit of incorporating total keratometry measurements in toric IOL calculations.
Additionally, cataract density can also impact the accuracy of optical biometry measurements, thereby influencing the precision of toric IOL power calculations. Optical biometry is preferred and considered the “gold standard” for its accuracy in most cases [27], with improved refractive outcomes compared to ultrasound biometry [28, 29]. However, some studies have shown that ultrasound biometry devices exhibit strong agreement with optical biometry devices in measuring axial length and anterior chamber depth, making them interchangeable in many clinical scenarios [30]. Although we excluded patients with extremely dense cataracts to ensure reliable measurements in this study, the accuracy of biometry in such challenging cases remains a real-world concern. Future research should continue to employ standardized cataract grading systems and consider incorporating advanced imaging techniques to improve measurement reliability.
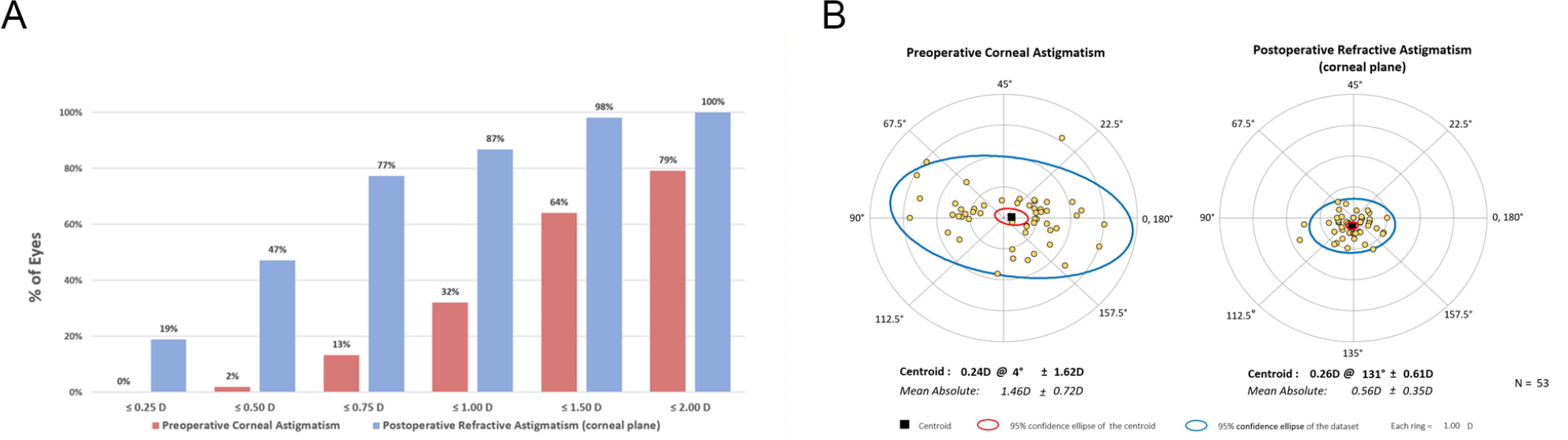
Vector analysis of the PE indicated that all calculators exhibited similar clustering patterns in double-angle plots, with the centroid of PE significantly different from zero. This systematic deviation from zero suggests that there may be common factors affecting all calculators, such as residual measurement errors or biological variability in wound healing and IOL positioning [31, 32]. Future research should focus on identifying and addressing these common sources of error to further improve toric IOL calculation accuracy.
Our study has several strengths, including the use of a single experienced surgeon, standardized surgical technique, and comprehensive evaluation of multiple modern toric IOL calculators. However, some limitations should be noted. The retrospective nature of the study and the relatively small sample size may limit the generalizability of our findings. Additionally, the actual implanted IOL axis and the axis recommended by the calculator may exhibit a slight difference, which, although typically minimal, could influence the interpretation of results. Also, due to the limitations of the current sample size, subgroup analysis based on astigmatism type or axial length was not performed. However, this could be a focus for future studies with a larger sample size. Finally, the one-month follow-up period, while clinically relevant, may not capture long-term refractive stability.
The performance of the six calculators in our study is comparable. While statistically significant differences were found between specific calculators (e.g., Barrett PPCA vs. Barrett TK), the magnitude of these differences may not translate to clinically meaningful outcomes for most patients. Surgeons may need to consider factors beyond predictive accuracy, such as ease of use, integration with existing systems, and specific patient characteristics, when selecting a toric IOL calculator. Future studies should focus on identifying patient subgroups or specific clinical scenarios where one calculator may outperform others. Prospective, multicenter studies with larger sample sizes and longer follow-up periods could provide more definitive evidence on the relative performance of these calculators. Additionally, investigating the impact of newer technologies, such as intraoperative aberrometry or artificial intelligence-based prediction models, could further advance the field of toric IOL calculations [31, 33].








留言 (0)