Morphometry of the optic nerve neuroretinal rim tissue is an essential element in the evaluation of glaucoma progression. SD-OCT of the ONH can be considered a widely used clinical standard today. After glaucoma surgery, in particular after filtration surgery, the evaluation of the morphometry of the ONH in SD-OCT can be a challenge. The effect of the structural reversal of disc cupping corresponding to an increase of the neuroretinal rim tissue thickness after surgery, has already been demonstrated for traditional filtration surgery, such as trabeculectomy. Several studies measured SRDC both for CSLT and SD-OCT imaging. Also, this effect has been shown for glaucoma drainage device surgery [22]. Up to now, to our knowledge, no studies exist, which quantify this effect for so-called minimally invasive bleb surgery (MIBS).
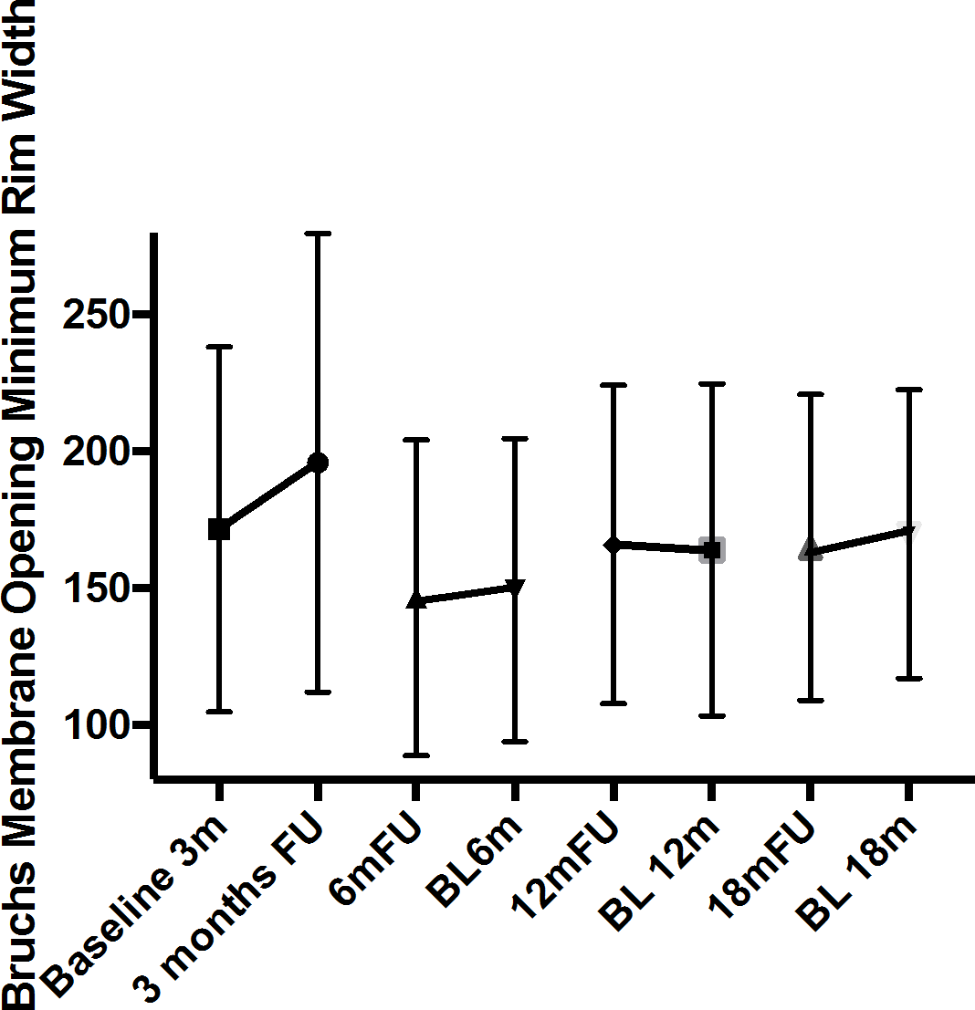
In this study we could show a significant increase in BMO-MRW in a short-term FU period of three months for MIBS surgery with the PRESERFLO® microshunt. When analyzing longer follow-up periods of 6–18 months, no significant changes in BMO-MRW were observed. The peripapillary retinal nerve fiber layer thickness remained unchanged in early follow-up. This is consistent with observations after trabeculectomy [7].
Morphometry of the ONH is known to be influenced by IOP changes in both ways. SD-OCT imaging allows quantification of the effect [23, 24]. The substantial decrease in IOP after filtration surgery is currently considered to be the main cause of SRDC [25]. Some studies suggest strong IOP fluctuations have less or no effect on pRNFL thickness [23]. This parameter’s higher independence from IOP fluctuations allows more stable and more unbiased morphometric glaucoma progression analysis compared to BMO-based parameters [3].
The correlation between IOP and BMO-MRW is especially known for cases with strong IOP changes after filtration surgery [21, 22, 25]. Normal diurnal surgery-independent IOP fluctuations however, do not seem to have any effect on the SD-OCT parameters BMO-MRW and peripapillary RNFL thickness [4]. It is not yet sufficiently known at which IOP decrease a measurable SRDC is detectable.
ICare rebound tonometry was used according to the departments SOP in order to increase patients comfort and to reduce the risk of postoperative infection. A meta-analysis of 147 publications, including 672 eyes, revealed a meta-difference (Icare® PRO-Goldmann applanation tonometry) of − 0.14 mmHg, indicating a non-significant, clinically irrelevant mean deviation (p = 0.335) [26].
With regard to the duration of SRDC, the results of this study differ from previous observations after different types of filtrating surgery. Also, BMO-MRW’s relative increase of 5.4% in three months follow-ups was lower than the reported change of this parameter after trabeculectomy (11.6% ± 22.6%) [7]. In summary, this study describes a less persistent and less prominent pattern of SRDC after PRESERFLO® implantation. Several hypotheses could explain these findings: Early partial occlusion of the shunt aims to avoid early postoperative hypotony and increases IOP levels in early follow-up [14]. The absence of very low IOP levels early postoperatively could reduce the development of SRDC. Another explanation could be higher IOP levels after PRESERFLO® implantation at three months follow-up compared to trabeculectomy. To test this hypothesis, a direct, preferable prospective study comparing trabeculectomy and MIBS would be desirable. Postoperative hypotony occurred in only 5.1% of patients. The rate of early postoperative hypotony seems to be higher after trabeculectomy than after PRESERFLO® implantation with temporary intraluminal occlusion [14].
The dependency between BMO-MRW and BMO-area is well known and has been described in numerous publications and as by our group. This relationship exists because, with an increasing BMO area, the retinal nerve fibers are distributed over a larger horizontal vector area, resulting in a thinner circumferential measured rim width. BMO-MRW, in turn, as shown in this study, correlates with intraocular pressure (IOP) reduction in the context of SRDC. However, BMO area does not correlate with IOP reduction. This phenomenon can be explained by the fact that BMO-MRW includes not only a horizontal vector but also a vertical vector, which is the only component influenced by SRDC.
In this study, the absolute increase in BMO-MRW after three months was similar across subgroups with varying severity of glaucoma. Thus, the extent of SRDC may not depend on the baseline BMO-MRW thickness.
In mid-term follow-up of more than 6 months after PRESERFLO® implantation, this study did not find any significant BMO-MRW increase. One explanation could be a weaker IOP-lowering effect of MIBS surgery compared to trabeculectomy: in a prospective randomized multicenter study, the PRESERFLO® microshunt performed significantly weaker in IOP lowering after one year compared to trabeculectomy with mitomycin C (14.3 mmHg vs. 11.1 mmHg) [18]. In this study, the rate of success defined as “IOP below 14 mmHg” without drop-outs was 35% for the PRESERFLO® group and 56% for the trabeculectomy group.
Another prospective study of a total of 300 patients confirmed these findings with slightly higher IOP values after 1 year of follow-up for the PRESERFLO® stent. The mean IOP was 12.9 mmHg after PRESERFLO® implantation and 11.4 mmHg after trabeculectomy [16]. Our results can be classified similarly with an average IOP of 13.7 ± 4.6mmHg at 12 months and 13.1 ± 4.5mmHg at 18 months after PRESERFLO® implantation. In our study, we found an early significant reduction of peripapillary RNFL thickness 6 months after PRESERFLO® implantation. After trabeculectomy, our previous study reported a significant RNFL thickness reduction only after 18 months postoperatively [7]. Interestingly, the amount of RNFL loss (PRESERFLO® -4.6 μm vs. trabeculectomy − 4.2 μm) was comparable at 18 months after surgery for both surgical approaches.
A stronger SRDC after trabeculectomy affecting also peripapillary RNFL thickness during the early postoperative period and potentially masking the retinal nerve fibre loss could be the reason to explain this difference between the effect after trabeculectomy and PRESERFLO® implantation:
Existing literature on SRDC has demonstrated neither a significant increase or decrease in RNFL in the early postoperative period after trabeculectomy (12 months postoperative). In contrast, this study identified a significant decrease already after the 6 months interval after shunt implantation. We therefore hypothesize that an early RNFL loss as measured for PRESERFLO may be masked by SRDC following trabeculectomy. Due to the reduction of the SRDC effect with time, the same RNFL reduction is measured after 18 months.
The tendency for a significant correlation between absolute IOP and RNFL reduction 18 months after PRESERFLO® implantation indicates that the level of long-term postoperative IOP may be crucial for the prognosis of postoperative glaucoma progression. Correspondingly, Koenig et al. reported a significant correlation between the postoperative IOP one year after filtrating surgery and the rate of progression of visual field defects [27].
Glaucoma progression as loss of neuroretinal tissue can occur focally. Therefore, the sectoral data of the OCT imaging data is crucial for structural progression analysis. Our work showed a reduction in RNFL thickness in various sectors after 3, 6, 12, and 18 months. A significant reduction in BMO-MRW was detected only in the temporal-inferior sector after 18 months. As SRDC biases BMO-MRW sectoral thicknesses for up to 18 months postoperatively, peripapillary RNFL thickness seems more suitable for an accurate assessment of glaucoma progression during this period after PRESERFLO® implantation.
The limitations of our study were the retrospective study design. It is important to consider that patients who did not have complicating events may have been less likely to come to tertiary care centers for follow-up examination. Patients with adverse events like hypotony could therefore be overrepresented in the early postoperative phase and amplify the effect. Furthermore, within the context of the retrospective study design, it was necessary to define certain follow-up groups. Nevertheless, this study may provide important additional information that is clinically relevant for the evaluation of glaucoma progression after PRESERFLO® implantation.
Furthermore, the study is limited by the lack of a control group. Previous studies have analyzed the fellow eyes’ course of BMO-based morphometry (BMO-MRW, BMO-MRA, RNFL-Thickness) following filtering surgery (glaucoma drainage device, trabeculectomy) and found no significant changes at any interval (1 week, 3, 6, 12, 18 months).
Another limitation of this study may be the exclusion of the 81 patients, which could lead to selection bias. In most cases, follow-up data were missing. This study aimed to assess real-world data to provide a basis for further clinical decisions.
Considering our results, PRESERFLO® implantation with primary temporary occlusion causes a significant transient SRDC. The phenomenon seems to be attenuated and of shorter duration when compared to trabeculectomy. The extent of SRDC may be associated with subclinical early hypotony after surgery.








留言 (0)