Patient selection
This retrospective cohort study was approved by the institutional review board of our tertiary hospital. The requirement for informed consent was waived because of the retrospective nature of the study (research number: 23-R001).
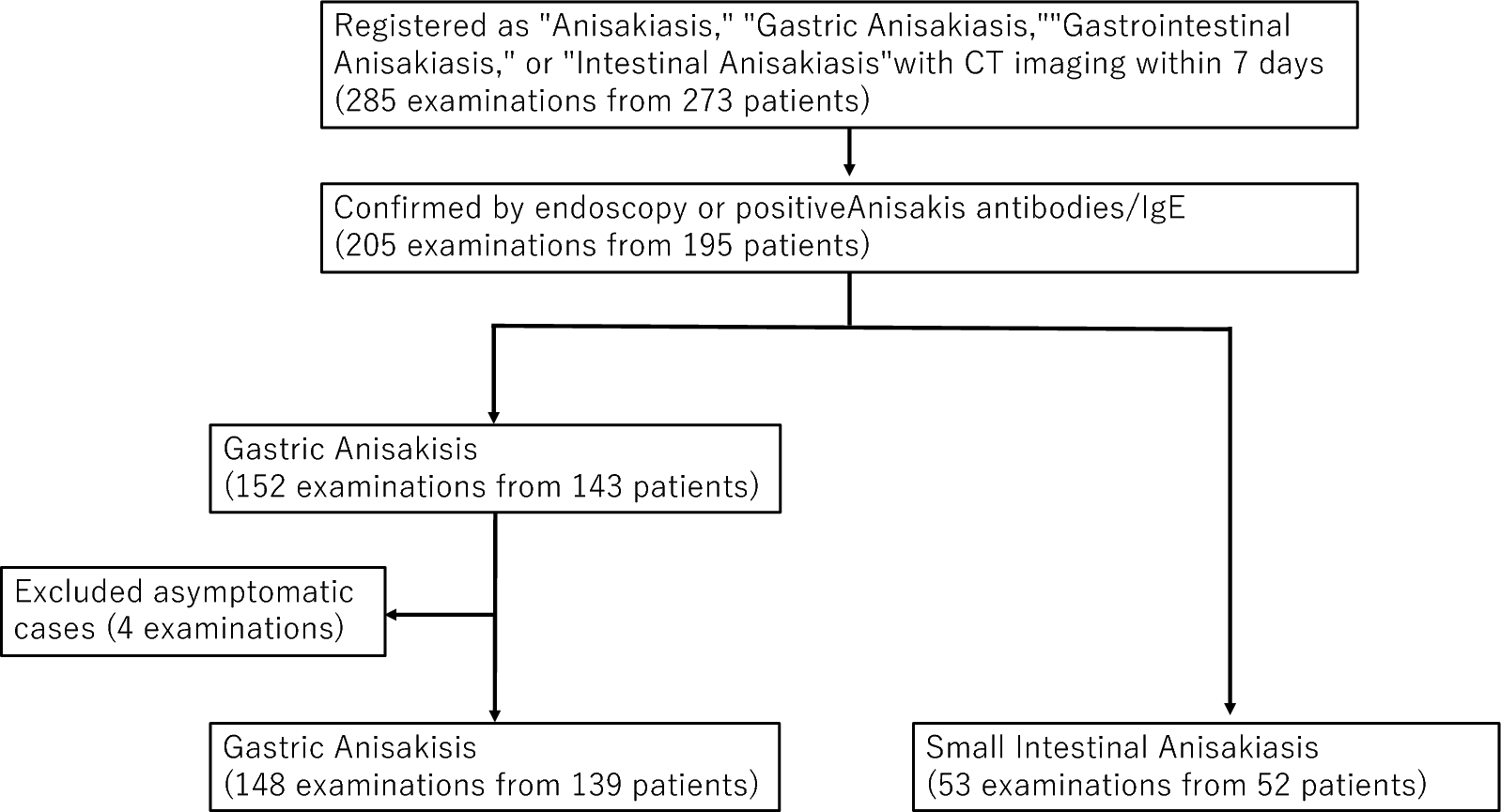
For the anisakiasis group, using electronic medical records, we initially extracted 285 examinations from 273 patients (10 patients with two examinations and one patient with three examinations) who were registered in medical records with diagnoses of “anisakiasis,” “gastric anisakiasis,” “gastrointestinal anisakiasis,” or “intestinal anisakiasis” and underwent CT imaging of the abdomen within 7 days before or after diagnosis registration. Among these, 205 examinations from 195 patients (eight patients with two examinations and one patient with three examinations) were confirmed either by direct visualization of Anisakis larvae via endoscopy or by testing positive for Anisakis antibodies or Anisakis-specific IgE. Cases were classified as gastric anisakiasis when confirmed by endoscopy, while those positive for Anisakis antibodies or Anisakis-specific IgE were classified as either gastric or small intestinal anisakiasis based on medical record review. This yielded 152 gastric anisakiasis examinations (from 143 patients: seven patients with two examinations and one patient with three examinations) and 53 small intestinal anisakiasis examinations (from 52 patients: one patient with two examinations). After excluding 4 asymptomatic cases that were incidentally discovered during endoscopy and showed minimal imaging findings, 148 gastric anisakiasis examinations (from 139 patients: seven patients with two examinations and one patient with three examinations) and 53 small intestinal anisakiasis examinations (from 52 patients: one patient with two examinations) remained.
For the gastric ulcer control group, using the same method, we initially extracted 215 examinations from 214 patients (one patient with two examinations) who were registered in medical records with “gastric ulcer,” tested positive for Helicobacter pylori, and underwent CT imaging within 7 days before or after diagnosis registration. We excluded cases with different final diagnoses (36 examinations), those where the abdomen was not included in the CT scan range (2 examinations), and those without endoscopic confirmation of gastric ulcer within 2 weeks before or after diagnosis registration (47 examinations). This resulted in 130 examinations from 130 patients, all of whom were symptomatic.
For the Crohn’s disease control group, similarly, we initially extracted 51 patients registered in medical records with “Crohn’s disease” who underwent abdominal CT imaging within 7 days before or after diagnosis registration. After excluding asymptomatic and post-surgical cases, 35 patients remained. Further excluding cases without clinical diagnosis of small bowel inflammation resulted in 27 patients. Although these patients were initially registered with Crohn’s disease only once, three patients underwent multiple CT examinations during subsequent symptomatic episodes (two patients with two examinations and one patient with three examinations), resulting in 31 examinations from 27 patients.
Image acquisition
Owing to the extended duration of the study, multiple CT scanners were used, including scanners manufactured by Canon Medical Systems Corporation (Aquilion ONE and Aquilion64) and GE Healthcare (HiSpeed NX/i, BrightSpeed Elite, LightSpeed RT16, Revolution CT, Optima CT660 Pro, and Revolution Maxima CT).
Unenhanced CT data were available for 64 examinations: 50 for gastric anisakiasis, 12 for gastric ulcers, 1 for small intestinal anisakiasis, and 1 for Crohn’s disease. Contrast-enhanced CT data were available for 301 examinations: 98 for gastric anisakiasis, 118 for gastric ulcers, 52 for small intestinal anisakiasis, and 30 for Crohn’s disease.
Contrast-enhanced images were obtained 90 s after intravenous administration of contrast media (80–135 mL of 300–350 mg/mL non-ionic contrast media, depending on the patient’s body weight). Reconstructed images with a 1.25–5 mm slice thickness were used for assessment.
Image analysis
Based on the radiological findings of previous studies, case reports [6,7,8, 10,11,12,13,14], and the clinical experience of our institution, the following radiological features were assessed:
Gastric lesions: Edematous thickening of the stomach wall, localized protrusion of the gastric wall, increased perigastric fat density, ascites, edematous changes in other bowel segments (small intestine and colon), fluid collection around the esophagus, and esophageal wall thickening.
Small intestinal lesions: Small intestine wall thickening, submucosal edema (target sign) in the small intestine, increased density of surrounding fat tissue, intestinal dilatation, clamp sign (progressive thickening of intestinal wall at the site of caliber change), and ascites.
The intestines were classified as “dilated” when the bowel lumen was > 3 cm, measured from one outer wall to the opposite outer wall. The clamp sign was defined as a gradual thickening of the intestinal wall at the transition point between dilated and non-dilated bowel segments, as described by Chen et al. [14]. Two radiologists with six (K.I.) and nine (D.Y.) years of experience independently reviewed the CT images. In cases of differing assessments, an abdominal radiologist with 18 years of experience (N.M.) reviewed the images to reach a consensus.
Clinical information
For all 362 cases, we collected the following data from medical records: demographic information (age and sex); clinical symptoms (abdominal pain, hematochezia, loss of appetite, hematemesis, fever, rash, nausea or vomiting, and altered mental status); laboratory findings (results of white blood cell count [WBC], C-reactive protein levels [CRP], and blood eosinophil cell count [EOS]).
Statistical analysis
Given the retrospective nature of this study, a formal power calculation was not performed. Patients with unavailable data were excluded from the analysis. Data are presented as the mean ± standard deviation or median (range) for continuous variables, such as age and Ki-67, and as numbers (percentages) for categorical variables. We used the t-test and Mann–Whitney U test for continuous variables and the chi-square and Fisher’s exact tests for categorical variables. Continuous variables were verified by Shapiro–Wilk statistics. A p-value < 0.05 was considered statistically significant.
Interobserver agreement was assessed by using κ values and was interpreted as poor (κ < 0.20), fair (κ = 0.21–0.40), moderate (κ = 0.41–0.60), good (κ = 0.61–0.81), or excellent (κ = 0.81–1.00). All statistical analyses were performed (K.I.) using EZR4.3.1 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) [15].





留言 (0)