OSAHS has a significant impact on all the systems of the body. The consequences of untreated OSAHS are wide-ranging and are postulated to result from fragmented sleep, intermittent hypoxia, hypercapnia, intrathoracic pressure swings, and increased sympathetic nervous activity that accompany disordered breathing during sleep [18]. We found a correlation between disease severity and fat, bone and muscle indices in patients with OSAHS by studying PSG, BCA, DXA, CT and blood-related indices in patients with OSAHS.
In our study, FM, BFP, VFA and TFM were positively correlated with HI, AHI, ODI, and T90%, and negatively correlated with mean SpO2. TG was positively correlated with AHI and ODI. Several studies have confirmed the relationship between fat content and OSAHS [19, 20, 21, 22]. Visceral adipose tissue was a key risk factor for OSAHS, and the number of apnea and hypopnea events per hour of sleep was significantly associated with the size of the VFA, and patients with large VFA exhibited increased incidence of OSAHS [19, 20]. Exercise training significantly reduced BMI, BFP, neck circumference, total body weight, and AHI [21]. In the intermittent hypoxic environment of OSAHS, the production of lipids increased, and the clearance rate of lipids decreased, leading to excessive accumulation of residual lipids [22].
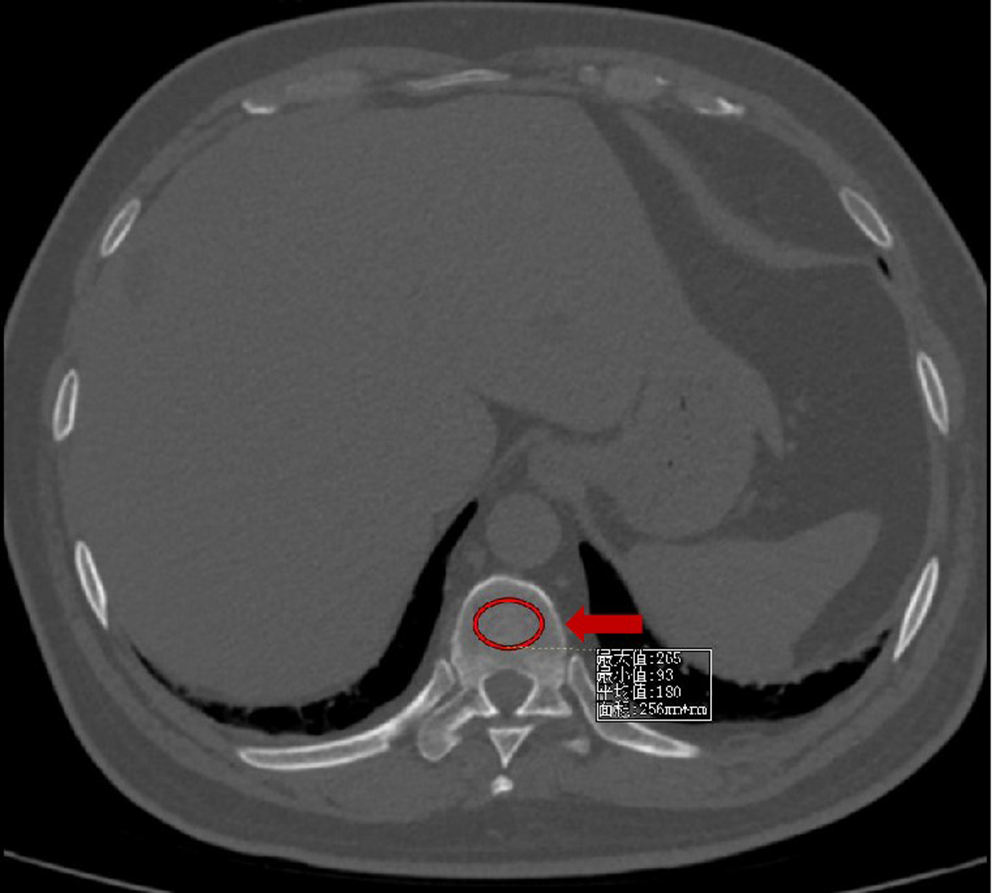
A meta-analysis showed that compared with that of the control group, the OSAHS group had a higher incidence of osteoporosis, lower lumbar spine BMD, and decreased lumbar spine T-score [10]. Another meta-analysis suggested that the odds of osteoporosis were higher in patients with OSAHS in cohort studies and lower in patients with OSAHS than in controls in cross-sectional studies [23]. These different results may be attributed to differences in population characteristics. In our study, T8, T9, T11, L1-CT values, mean vertebral CT values and 25(OH)D3 were positively correlated with mean SpO2 in patients with OSAHS. This was similar to the findings of a study that documented significant correlations between lower BMD in the lumbar spine and femur, and the alteration of night oxygen saturation indices in the male population, including lower mean arterial oxygen saturation (SaO2) and SaO2 nadir, and higher T90% [24]. This indicated that there was a correlation between hypoxia and osteopenia in patients with OSAHS. HIF-1α, which was elevated in hypoxia, directly induced osteoclastic bone resorption and downregulated osteogenic differentiation of mesenchymal stem cells [25, 26]. Bone destruction appeared to increase in rats exposed to cigarette smoke and intermittent hypoxia compared to those exposed to air, possibly owing to the heightened inflammation (IL-6 and TNF-α) [27]. Gene expression profiling revealed that potassium inwardly rectifying channel subfamily J member 1 (KCNJ1), natriuretic peptide receptor 3 (NPR3) and wilms tumor 1 antisense RNA (WT1-AS) were identified as shared diagnostic biomarkers of OSAHS and osteoporosis patients, all of which were associated with immune cell infiltration [28]. The etiology of bone resorption and osteopenia/osteoporosis in patients with OSAHS could be complex and multifactorial, including nocturnal hypoxia, immune dysfunction, alterations in vitamin D homeostasis, chronic systemic inflammation, and reduced physical activity related to sleepiness and obesity [24, 27, 28].
We hypothesized that patients with OSAHS would experience muscle loss. In our study, PMD negatively correlated with HI, AHI, ODI, and T90% and positively correlated with mean SpO2. This was consistent with Takeshi Matsumoto’s research showing that AHI correlated negatively with skeletal muscle density in both men and women [29], which suggested that more severe OSAHS was associated with greater fat accumulation in muscles. Neither PMA nor PMI were associated with sleep monitoring indices in our study. PMA and PMI were positively correlated with BMI respectively, while PMD was not correlated with BMI. Therefore, BMI might affect the relationship between PMA or PMI and sleep monitoring indices. In another study, high risk of OSAHS was associated with low muscle mass in participants aged ≥ 50 years and with low muscle strength among obese participants [13]. Stevens D found that reduced dominant hand grip strength (HGS) was associated with a lower oxygen nadir, greater time spent below 90% oxygen saturation, and increased apnea duration, suggesting that impairments in HGS may be related to fat infiltration of muscles, hypoxemia-induced reductions in peripheral neural innervation, or even endothelial dysfunction, which was a common outcome of hypoxemia [30].
Fat, bone, and muscle indices were used to predict the sleep monitoring measures. Multiple prediction models were established after correcting for the mixed factors. FM, BFP, VFA, TG and PMD were entered into the optimal multiple linear regression equations for AHI. TG was associated with AI. FM, PMD, T9, and L1 were associated with HI. These suggested that an increase in fat or decrease in PMD predicted a higher AHI or HI, and a decrease in vertebral CT value predicted a higher HI. For oxygen related indices, ASM, FM, BFP, VFA, WHR, TG, TC and PMD were entered into the optimal multiple linear regression equations for T90%. FM, VFA, TG and PMD were associated with the ODI. FM, BFP, VFA and 25(OH)D3 were associated with mean SPO2. These reflected that an increase in fat and decrease in ASM, PMD and 25(OH)D3 predicted worse SPO2. All these results indicated that fat, bone, and muscle indices were correlated with sleep monitoring measures to a certain extent, which could provide clinical guidance.
Our study also had some limitations. First, the sample size was relatively small. Second, this was a cross-sectional study, which could only explain the correlation between disease severity of OSAHS and fat, bone, and muscle indices, but could not explain causality. Third, the molecular mechanism has not yet been studied.
Increased fat content, decreased vertebral CT values, and decreased muscle mass and density were associated with higher AHI and T90%, reflecting a higher degree of OSAHS severity. Attention should be paid to the extrapulmonary effects in patients with OSAHS, such as changes in fat, bone, and muscle metabolism. Comprehensive monitoring should be conducted with BCA, DXA, CT and other examinations for the early detection and intervention of abnormalities to reduce the occurrence of obesity, osteoporosis, and sarcopenia. Intermittent hypoxia may affect the metabolism of fat, bone, and muscle in patients with OSAHS. However, further studies are needed to evaluate these connections.




留言 (0)