Study design
A quantitative, cross-sectional study.
Study setting and sampling
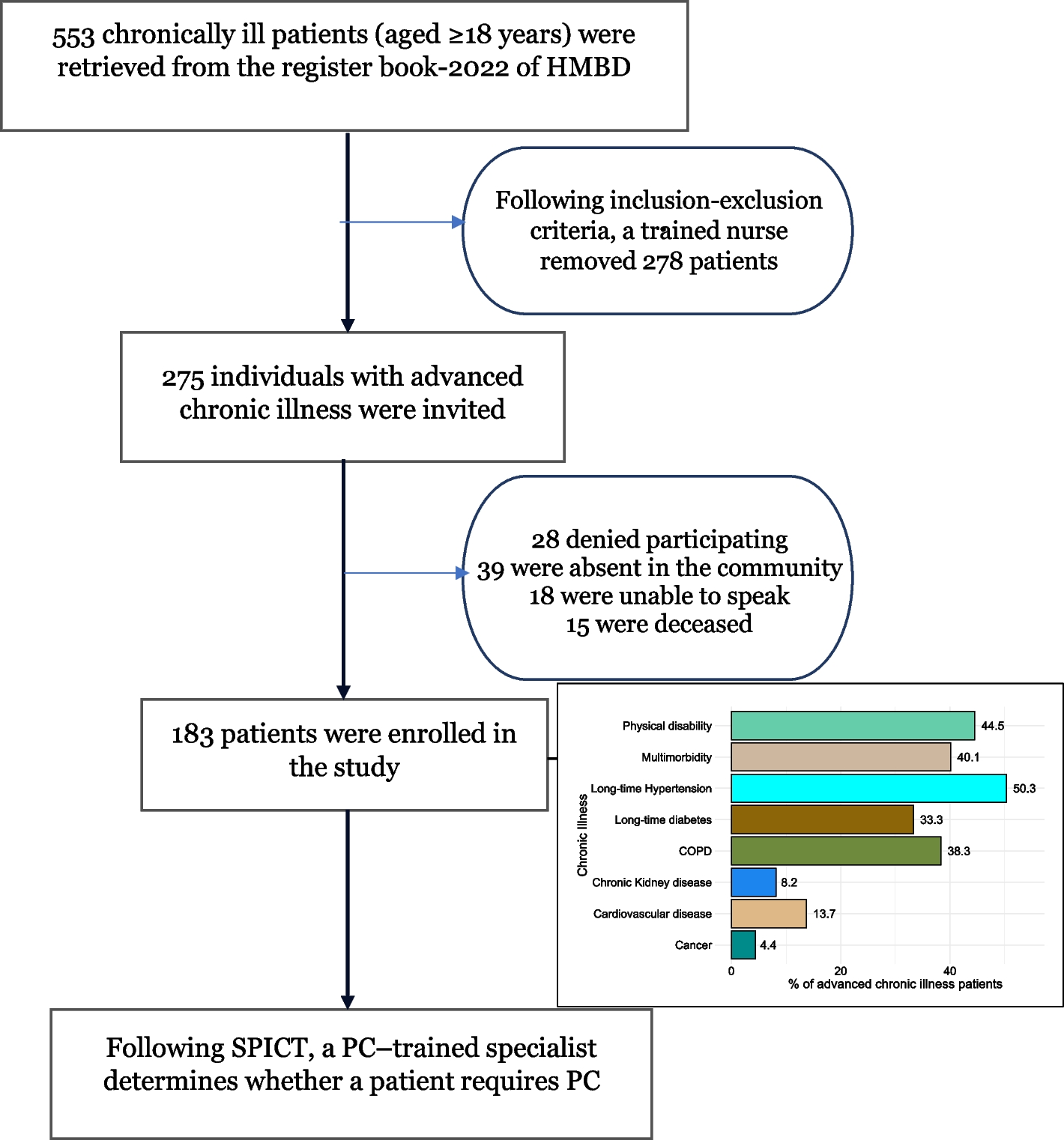
Random cluster sampling is a useful technique in cross-sectional studies, particularly when dealing with large, geographically dispersed populations or when it is impractical to survey individuals directly due to resource constraints. Therefore, this sampling method was used in this study. First, we coded the 34 provincial administrative regions in China and selected 5 provinces based on a random number table, and then coded the tertiary-level hospitals in each province and randomly selected 4 hospitals. Finally, ICU nurses from 5 hospitals in 4 provinces participated in this study between March and April of 2024. If a registered nurse had at least one year of ICU work experience and gave their agreement to participate, they were considered included. Nurses on sick or maternity leave were not included. Larger sample sizes in surveys are known to yield more accurate and representative results. According to MacCallum et al. [23], there should be a minimum required sample size of 100 or a minimum sample size to variable number ratio of 5, resulting in a final sample size range of 300 to 500 ICU nurses.
Measures
A four-part questionnaire, consisting of the demographic information, and Moral Distress Scale-Revised (MDS-R), the Attitude toward death Profile-Revised (DAP-R), Palliative Care Nurses’ Core Competences Scale (PCNCC) was used for data collection.
Demographic information
Including age, gender, work experiences, marital status, education status, position, region, palliative care-related education or training.
Moral distress scale-revised (MDS-R)
The 38-item MDS was first created by Corley et al. [24] and then amended to 21 items by Hamric et al. [25] The MDS-R uses a Likert scale to assess moral distress frequency, which goes from 0 (never) to 4 (very frequently), and present severity, which goes from 0 (none) to 4 (large extent). Each item score is obtained by multiplying the intensity and frequency scores. Total score ranges from 0 to 336. The moral distress will increase with a higher score. Sun et al. [26] translated the MDS-R in China. MDS-R in this study has a Cronbach’s alpha of 0.893.
Attitude toward death profile-revised (DAP-R)
The Attitude toward death Profile-Revised (DAP-R) is 32-item measure with five subscales: fear of death (negative), death avoidance (negative), neutral acceptance(positive), approach acceptance (positive), and escape acceptance (positive). Scores for positive or negative dimension are averaged by the number of items, and the scale does not calculate a total score but rather interprets attitudes based on individual dimension scores. Item with scores ranging from 1 (totally disagree) to 5 (totally agree), the total score is the sum of the scores for each attitude subscale, higher scores indicate a stronger tendency towards the attitude represented by each dimension [27]. Tang et al. [28] translated DAP-R in China. DAP-R in this study has a Cronbach’s alpha of 0.910.
Palliative care nurses’ core competences scale (PCNCC)
Palliative care nurses’ core competence scale was developed by Han [29] based on Competency outcome and performance assessment model (COPA), which includes 28 items across four dimensions: ethical care competency, physical and mental care competency, spiritual care competency, and self-psychological adjustment competency. Each item ranging from “not capable” to “very capable” for a total score of 0 to 112, with higher scores indicating a higher core competency. PCNCC in this study has a Cronbach’s alpha of 0.924, split-half reliability and retest reliabilities are 0.889 and 0.976, respectively.
Data collection
This study was conducted on online, which is called “wenjuanxing”, the largest e-questionnaire platform in China. Our research team contacted the directors of the nursing departments of 5 hospitals in 4 provinces and after explaining the study’s purpose, process and obtaining consent, the directors of the nursing departments sent the questionnaire URL link to the participants who met the inclusion criteria. The first page of the questionnaire described the study in detail and asked participants if they were willing to join, and only those who selected “Yes, I agree to join” were allowed to complete the rest of the questionnaire.
Data analysis
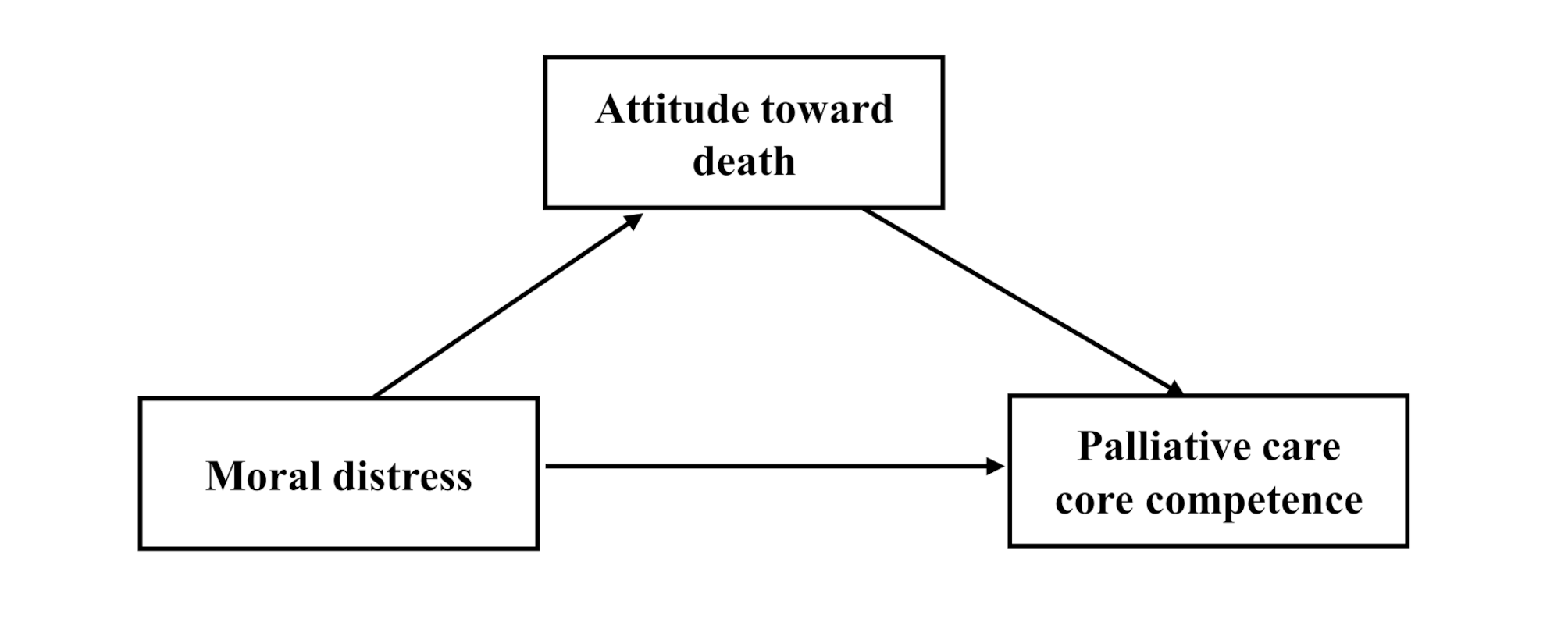
IBM SPSS ver. 19.0 were used. The variables and characteristics of the participants were described using descriptive statistics. The mediating effect was investigated using a stepwise regression analysis, and correlations between the variables were examined using Pearson’s coefficient. Step 1 involved regressing moral distress (independent variable) on palliative care core competencies (dependent variable). Step 2 involved regressing moral distress (independent variable) on palliative care core competencies. Step 3, palliative care core competencies was regressed on attitude toward death and moral distress. The link between moral distress and palliative care core competencies became less (partial) or non-significant (full) when put moral distress and attitude toward death into the regression model. This showed that the mediating effect was confirmed. The indirect effect was estimated using a bootstrap approach, which included a 95% CI. Model 4 was carried out with the Process macro. The p-value less than 0.05 indicates statistical significance.
Ethical consideration
The study was approved by The First Affiliated Hospital of Dali University (with the codes DFY20240403001). We explained the study’s purpose and process in the consent form, as well as the voluntary nature and anonymous. Lastly, all data were securely stored on a password-protected computer accessible only to team members.




留言 (0)