
記住我
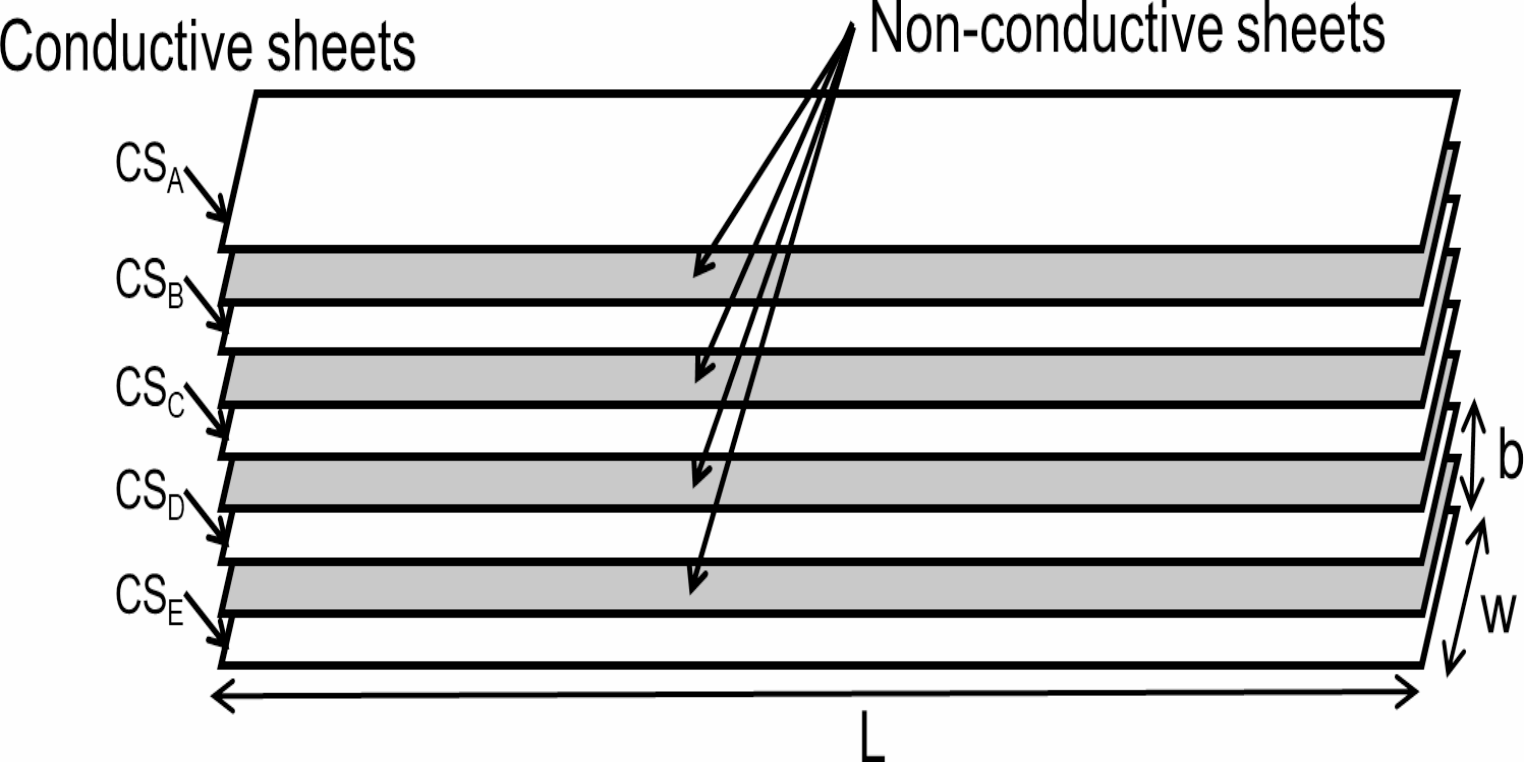








Figure 1 shows the layered structure of the bending angle sensor based on the double-layer capacitance technology. The sensor design is based on the one used in a previous study [32]. It comprises five layers, alternating between conductive (CSA to CSE) and nonconductive materials. The length of the sensor is more than 600 mm, which surpasses the typical half circumference of the rib cage and abdomen, ensuring comprehensive coverage. Its width is maintained at 20 mm to facilitate easy integration with smart clothing. The capacitance between successive conductive sheets is calculated using the following equation:
Fig. 1
Bending angle sensor based on double-layer capacitance. Structure of the bending angle sensor, featuring five conductive layers separated by nonconductive layers. The dimensions of the sensor are 600 mm × 20 mm (length (L) × width (W))
$$\:\beginC=__\frac,\end$$
(1)
where C is the capacitance, \(\:_\) and \(\:_\:\)are the permittivity of vacuum and a nonconductive sheet, respectively, l is the length, w is the width, and b is distance between successive conductive sheets. Consider a micro-interval section ds in which the angle between both ends of the pair of conductive sheets is θ and the deformation is discretionary (Fig. 2a). When the radius of curvature in the micro-interval is r(s) from one end to a length s, each conductive sheet is distorted by a length change rate of \(\:_\) and \(\:_\) in the micro-interval ds. The two distortions, assuming that they are on a circular arc as shown in Fig. 2b, can be computed using the following equations:
Fig. 2
Illustration of bending angle and capacitance variation. (a) The entirety of conductive sheets and (b) Enlarged view of the micro-interval section
$$\:\begin_=\frac_-ds}=\frac,\:\:\end$$
(2)
$$\:\begin_=\frac_-ds}=-\frac,\:\end$$
(3)
where \(\:_\) and \(\:_\) are the length change rate. The expansion and contraction rates \(\:l}_\) and \(\:l}_\) for the entire measurement section can be obtained by integrating \(\:_\) and \(\:_\), respectively.
$$ \begin l_ & = \mathop \int \limits_^ \varepsilon _ ds = \mathop \int \limits_^ \frac}r\left( s \right)d\theta \\ & = \frac\theta, \\ \end $$
(4)
$$ \begin }l_ = & \mathop \int \limits_^ \varepsilon _ ds = \mathop \int \limits_^ - \frac}r\left( s \right)d\theta \\ = & - \frac\theta, \\ \end $$
(5)
Therefore, regardless of the shape of the deformation of the conductive sheet, the amount of expansion and contraction is proportional to the angle θ between the two ends. As shown in Eq. (1), since the capacitance is proportional to the length of the conductive sheet, the capacitance is also proportional to the angle θ between the two ends, regardless of the shape of the deformation of the conductive sheet.
$$ \begin \Delta C &= \varepsilon _ \varepsilon _ \frac}l_ } \right)}} - \varepsilon _ \varepsilon _ \frac}l_ } \right)}} \\ &= 2\varepsilon _ \varepsilon _ w\theta, \\ \end $$
(6)
Therefore, only the bending angle θ can be measured accurately even if the conductive sheet is wrinkled. In this study, the conductive sheet has a five-layer structure, and the capacitance between each layer is CA−B, CB−C, CC−D, and CD−E. The uppermost surface CSA and the lowermost surface CSE are connected to the ground (GND) of the measurement circuit to isolate the capacitance of the sensor from the influence of the human body and environmental potentials. Therefore, the capacitance difference (ΔC) between the parallel capacitances of CA−B and CB−C (CU) and CC−D and CD−E (CL) is measured. Even if the bending angle sensor is compressed or stretched, ΔC is not affected because CU and CL change in identical manner. The bending angle sensor of the double-layer capacitance method can accurately measure only the bending angle θ, independent of the shape change due to length, pressure, or wrinkle.
2.2 Smart clothing for respiratory rate monitoringFigure 3 shows a low compression smart clothing integrated with the proposed bending angle sensor. In a previous study, changes in the body shape in the rib cage and abdomen regions during resting breathing were found to vary with posture [33]. For this reason, in the present study, the bending angle sensors were strategically positioned at the height of the rib cage and abdomen, extending from the center of the front side to the back, to optimize the detection of respiratory movements. The measurement circuit box was centrally located on the front side of the garment. The bending angle sensor and measurement circuit box were attached to the underwear using double-sided tape.
Fig. 3
Illustration of smart clothing equipped with a bending angle sensor based on double-layer capacitance
Figure 4 shows a schematic of the alterations in body shape during respiration, as viewed in a horizontal cross-section. The bold line represents the sensor, whereas the solid and dashed lines represent the body contours during inhalation and exhalation, respectively. Notably, the double-layer capacitive-type bending angle sensor used in this research can measure the bending angle θ at both ends without being affected by the shape change in the middle of the sensor; therefore, there is no need to consider the shape in the middle of the sensor despite the proposed low-pressure smart garment causing wrinkles in the bending angle sensor. Furthermore, the sensor length (L) remains constant despite variations in body shape caused by breathing because the tension in the sensor exceeds the wearing pressure. This results in a shift of the position of the sensor from A-B during exhalation to A-B’ during inhalation. Accordingly, the angle of the sensor changes from \(\:_\) to \(\:_\) owing to respiratory movements. The corresponding change in capacitance induced by breathing, denoted as \(\:\varDelta\:_\), is quantified using Eq. (7).
Fig. 4
Schematic illustrating the bending angle sensor based on double-layer capacitance responding to changes in body shape owing to breathing. The solid line represents the body shape at exhalation, and the dashed line represents the expanded body shape at inhalation. The bending angle of the sensor changes accordingly from θC to θE
$$\:\begin\varDelta\:_=2__w\left(_-_\right)\end$$
(7)
2.3 Respiratory rate monitoring systemFigure 5 shows the experimental setup and measurement block diagram. The sensor output signals from the smart clothing positioned at the rib cage and abdomen, along with the ventilation volumes from the spirometer, were simultaneously recorded on a PC through an analog-to-digital (AD) converter (NI USB-6128, National Instruments) at a sampling frequency of 100 Hz. Simultaneously, ventilation volume was measured using an electronic spirometry system equipped with a gas analyzer (AE-310 S, Minato Medical Science, Osaka, Japan). In addition, a metronome controlled via a PC indicated the respiration timing. The compressive pressure exerted by the sensors on the thorax was measured using the airbag method [34]. This setup was used to monitor the respiratory rate in different postures.
Fig. 5
Illustration of experimental setup and measurement block diagram. (a) An example of measurement in the sitting posture. Pressure meter and air bag are used only initially and removed before the respiratory rate measurement. (b) Measurement block diagram for respiratory rate monitoring, featuring the bending angle sensor based on double-layer capacitance coupled with a CV converter
Figure 5b shows the respiratory rate monitoring system that incorporates the bending angle sensor. In this system, the capacitance of the sensor is converted into voltage via a capacitance-to-voltage (CV) converter. The conductive sheets CSA, CSC, and CSE of the sensor are connected to the ground (GND) of the CV converter. The CV converter applies a 10 kHz pulse wave through resistors R1 and R2 to the sensor. The charge and discharge voltages are fed into an instrumentation amplifier (IA) and subsequently processed through a half-wave rectifier circuit and a low-pass filter (LPF), which has a cutoff frequency above 10 Hz. The resulting output signal (OUT1) translates the differences in parallel capacitance between CA−B+CB−C and CC−D+CD−E into voltage, capable of detecting both positive and negative bending angles of the sensor. The output signal for respiratory detection (OUT2) undergoes further signal processing, including DC cut and amplification to enhance its reliability and accuracy.
2.4 Signal processingBending angle sensors also pick nonrespiratory signals, such as body motion. Therefore, at the onset of the signal processing, we identified periods affected by body motion in the sensor output to prevent false detections. High-pass filter (HPF) processing with a cutoff frequency of 3 Hz, which can attenuate respiratory signal components of 0.2–0.5 Hz to 1/10 or less, was applied to the ADC1 signals obtained from the rib cage and abdomen sensors to detect noise related to body movements. Periods influenced by body motion were designated as 1 s before and after the detection of an amplitude exceeding a predefined threshold value post-HPF processing. Subsequently, band-pass Filter (BPF) processing with a frequency range of 0.2–0.5 Hz, which is the respiratory frequency measurement range, was applied to the ADC2 signals obtained from the rib cage and abdomen sensors. During this stage, periods influenced by body motion were ignored by treating them as no-signal periods. In this case, the period affected by body motion was ignored as a no-signal period. Because the chest and abdominal movements due to breathing in normal subjects are synchronized [35], to stabilize the waveform, we averaged the signals from the rib cage and abdomen to reduce the noise occurring specifically in the thorax or abdomen. However, because the amplitude of each sensor signal was different, we normalized the signals obtained from both the thorax and abdomen after BPF processing and then generated the ensemble waveform. The expiratory and inspiratory phases were identified within the ensemble waveform using the zero-crossing method [10]. This study aimed to measure the respiratory rate at rest and it was calculated using a moving average of the detected respiratory intervals. A three-point moving average was used wherein the difference of respiratory rate within the moving average points was within ±1 bpm owing to the use of the metronome to cue the respiratory rate acceleration by 1/3 bpm with each breath. For comparison, the respiratory rate was also estimated from the respiratory waveform obtained using the spirometer. The amplitude of the ensemble waveform at each breath was also computed.
2.5 Subjects and experimental procedureTwenty healthy male subjects without any respiratory diseases, including asthma and COPD, participated in this study to evaluate the performance of respiratory rate measurement using smart clothing. The study received ethical clearance from the Ethical Review Committee of Ritsumeikan University (Approval number BKC-LSMH-2022-072), and all participants provided informed consent prior to participation. Details regarding the subjects are summarized in Table 1.
Table 1 Subject informationInitially, all subjects wore the smart clothing, and the compression pressure exerted by the sensor at the rib cage was assessed using the air bag method [34]. The compression pressure under the smart clothing at the rib cage sensor was measured using a Φ15-mm air bag to be in the range 0.05–2.00 kPa. Subjects also verbally confirmed whether they experienced any discomfort due to the compression pressure. Subsequently, participants were instructed to breathe for approximately 3 min in sitting, supine, and lateral postures, synchronized with a metronome controlled via a PC that gradually increased the respiratory rate from 12 bpm to 30 bpm. The lateral position was defined as the position where the bending angle sensor was placed between the bed and body. Because the sensor was under pressure, this configuration was selected as a more severe condition than that in the opposite direction.
The measurement accuracy was assessed through a Bland–Altman analysis, which compared the respiratory rates derived from the low compression smart clothing and the spirometer to find out the similarity. Furthermore, the mean absolute error (MAE) and mean absolute percentage error (MAPE) were used as additional error measures to show the normalized errors. According to a previous study [36], the 95% limits of agreement for respiratory rate measurements by the same, different, and simultaneous observers were −4.86 to 4.94 bpm, −5.7 to 5.7 bpm, and −4.2 to 4.4 bpm, respectively. In this study, we calculated the percentage of respiratory rates that fell within a 4 bpm error margin. Additionally, to explore the relationship between compression pressure and measurement error, we compared the pressure against the mean limit of agreement (LOA) across all postures for each subject. The Pearson correlation coefficient was utilized to determine statistical significance, with a threshold of p < 0.05 for significant results.
留言 (0)