
記住我






Overall, 1221 patients were registered at the practice during data collection (Table 1). Males comprised the majority of the population (84.9%) and the population had a mean age of 39.7 ± 12.2 years and a mean time registered with the practice of 3.9 ± 4.3 years. Asylum seekers accounted for 14.5% of the patients. Based on their current address, 86 (7.0%) of patients were recorded has having no fixed abode, 152 (12.4%) in a hostel, 167 (13.7%) in a hotel, 88 (7.2%) in supported accommodation and the remaining 645 (52.8%) had a residential address recorded that represented some form of temporary accommodation (permanent living situations do not remain at the specialist practice). Of the total population, 319 (26.1%) were recorded as rough sleeping at some point.
Table 1 Characteristics and differences between those with a non-fatal overdose and those withoutA total of 462 (37.8%) had at least one chronic condition reported. Of the conditions included, blood-borne viruses (BBV) were recorded in 167 (13.7%) of the population, and respiratory conditions were recorded in 145 (11.9%). There was a high prevalence of mental health conditions within the population, with 619 (50.7%) having at least one mental health condition documented. Depression was the most common (n = 410, 33.6%), followed by anxiety (n = 276, 22.6%). An attempt at suicide or self-harm at any time had been recorded in 185 (15.2%).
Substance useCurrent smokers made up 55.7% (n = 680) of the total patient group, and 44.2% (n = 540) were recorded as consuming alcohol. This included 265 (21.7%) noted to be problem drinkers.
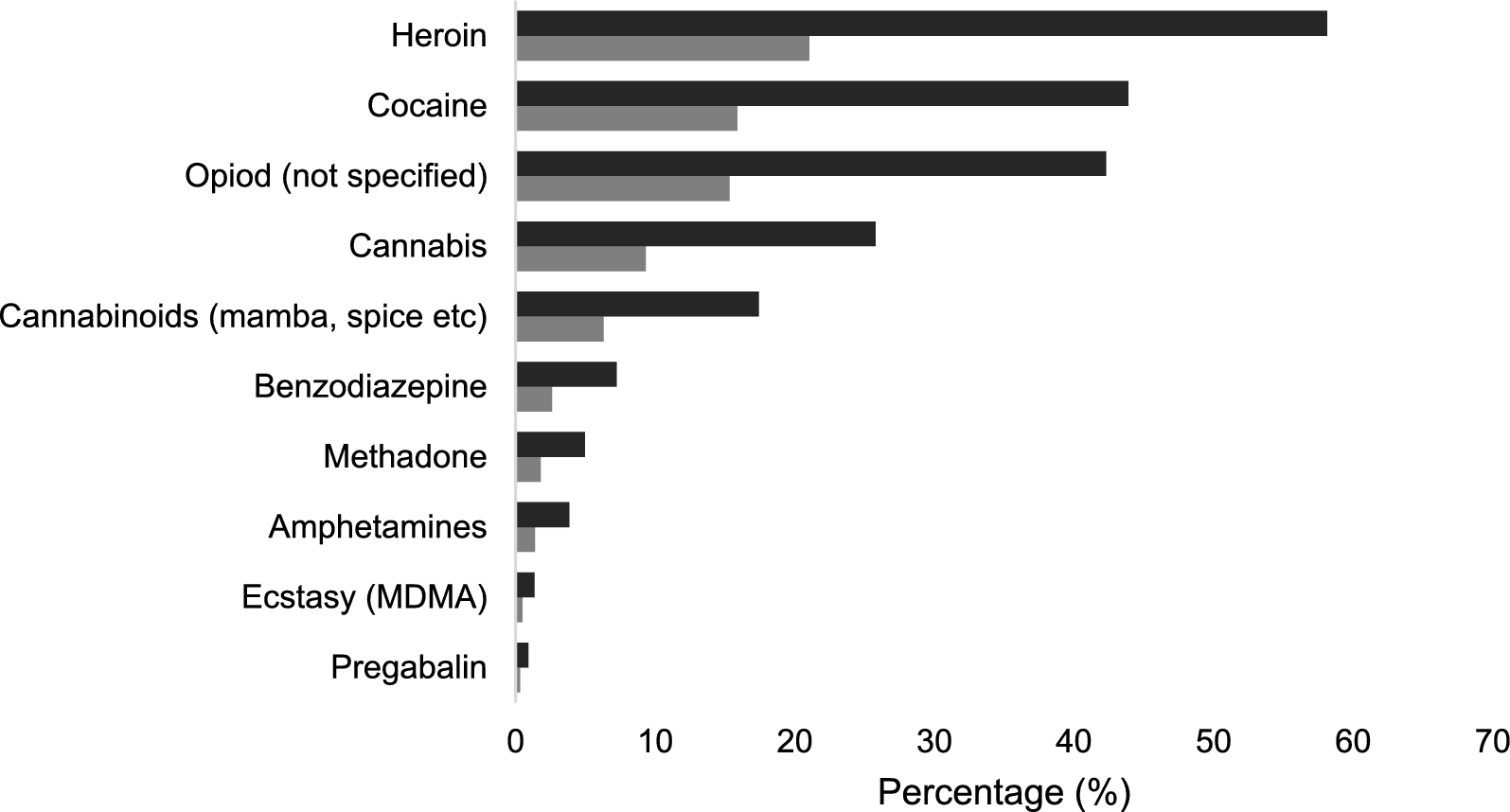
Illegal substance misuse was identified in 442 patients (36.2%). Heroin was the most common substance of use, with 257 (58.1%) of the substance misuse population reported as users (21.0% of the total population). As shown in Fig. 1, other common substances included cocaine (194, 43.9% substance misuse population; 15.9% total population), cannabis (25.8% of substance misuse population, 9.3% total population) and synthetic cannabinoids such as mamba and spice (n = 77, 17.4% substance misuse, 6.3% total population).
Fig. 1
Substance of use in all patients with coded substance misuse (n = 442). Percentages represent that of the substance misuse population, n = 442 (dark grey) and the total population, n = 1221 (light grey). Methadone refers to the misuse of methadone, not prescribed use
Non-fatal overdosesIn total, 194 patients (15.9%) were recorded as ever having had a NFOD, with 428 overdoses between them. The median number of overdoses was 1, with 100 patients (51.5% of patients with NFOD) having just one recorded episode. Two overdoses were recorded in 45 people (23.2% of patients with NFOD), three in 22 people (11.3% of patients with NFOD), four in 12 people (6.2% of patients with NFOD) and 15 people (7.6% of patients with NFOD) had 5 or more overdoses recorded. The maximum number of episodes recorded for a single patient was 21. In the five years prior to the data collection, 94 patients (7.7% of all patients) had a recorded overdose.
No information beyond the coded term of substance overdose was available for 121 (28.2%) of the 428 overdoses. In total, there were 264 (61.7%) incidents that had a recorded substance of overdose, and 208 (48.6%) had information regarding the management.
Substance of overdoseOf the 264 NFODs that had a substance recorded, single substance overdoses were seen in exactly half (50.0%) of these, with poly-substance overdoses accounting for the other half. Alcohol use was implicated in a further 51 (19.3%) of these overdoses.
As seen in Fig. 2, for single substance overdoses (n = 132), the most commonly identified substances were: heroin (n = 30, 22.7%), paracetamol (n = 30, 22.7%), synthetic cannabinoids (n = 9, 6.8%), SSRIs (n = 9 6.8%), anti-psychotics (n = 7, 5.3%), benzodiazepines (n = 7, 5.3%) and co-codamol (n = 5, 3.8%). For polysubstance overdoses, paracetamol (n = 37, 28.0%) was the most common substance followed by heroin (n = 31, 23.5%), cocaine (n = 32, 24.2%), benzodiazepines (n = 31, 23.5%), anti-psychotics (n = 21, 15.9%), SSRIs (n = 19, 14.4%), mirtazapine (n = 18, 13.6%), synthetic cannabinoids (n = 16, 12.1%), pregabalin (n = 16, 12.1%), sleeping tablets – unspecified, but could include benzodiazepines (n = 16, 12.1%), co-codamol (n = 13, 9.8%) and methadone (n = 13, 9.8%).
Fig. 2
Substance of overdose for 264 overdoses of known substances. (Full bar length = overall total, broken down for polydrug overdoses (dark grey) and single drug overdoses (light grey))
Of the 194 who had a recorded overdose, 146 (75.3%) had coded substance abuse on record. Heroin was the most common substance of use, with 91 (46.9% NFOD population) reported to be users. Other opioids not specified (n = 74, 37.6%), cocaine (n = 54, 37.1%), cannabis (n = 37, 19.1%), synthetic cannabinoids (n = 28, 14.4%) and benzodiazepines (n = 22, 11.3%) were also popular substances of abuse.
Use of emergency services in NFODOf the 208 overdoses with management information, 110 (52.9%) had an ambulance call out (Table 2). Of these, 21 (10.1%) involved the patient self-discharging from the ambulance prior to reaching the hospital. Naloxone was administered in 32 (15.4%) cases, primarily given by the ambulance service. Overall, 148 (71.2%) NFODs led to a presentation to the ED, with self-discharge before assessment in 21 cases (10.1%).
Table 2 Services used for non-fatal overdoses (total = 428 overdoses)In total, 57 overdose events (27.4%) led to hospital admissions. For 25 of these 57, a length of stay was recorded. The majority (n = 14) stayed for one day, 7 for two days, two individuals for 3 days, one person for 4 days, one for 11 days and one for 25 days. The short single-day stays were reported for observation, whereas longer stays were due to co-existing issues, including aspiration pneumonia (25 days), mental health reasons (11 days) and leg ulcers (3 days).
Circumstances leading to NFODIn some of the medical notes, there was descriptive text regarding the overdose. In general, two subsets of overdoses appeared. Firstly, was the group that intended to self-harm or attempt suicide. In 50 cases (12% of NFODs with available data), direct references to mental health were made, with 25 (9% of NFODs with available data) noting suicidal intent. These were often triggered by life events such as relationship breakups or a family member dying. These overdoses often involved taking multiple different street substances and/or prescribed medications.
A second subset (n = 91, 44% of NFOD with available data) involved regular substance users who overdosed on street drugs. This group appeared more likely to self-discharge from emergency care. Of 91 overdoses identified as caused by street drugs (predominantly heroin and cocaine), self-discharge from ambulances or ED occurred in 31 (34.1%) cases accounting for 73.8% of the self-discharge events. While it is not possible to be certain, many overdose events were likely unintentional due to factors such as reduced tolerance from being in prison noted.
Risk factors for non-fatal overdoseSeveral factors were associated with individuals with a recorded NFOD compared to those without (Table 3). Male sex was associated with a reduced risk of NFOD (OR: 0.52, 95% CI 0.33–0.81), white ethnicity a greater risk compared to Black/African/Caribbean (OR: 0.42, 95% CI 0.21–0.85) or Asian (OR: 0.42, 95% CI 0.20–0.89) and age 36–45 associated with higher risks (OR: 3.86, 95% CI 1.33–11.22).
Table 3 Factors associated with non-fatal overdoseBeing an ex or current smoker increased the odds of a NFOD by 5.45 (95% CI 1.41–21.00) and 10.84 (95% CI 3.84–30.58) times, respectively, as did being ever reported as an alcohol drinker (OR: 2.19, 95% CI 1.51–3.17). However, being non-alcohol dependent increased the likelihood of NFOD compared to a reported alcohol dependence (OR: 2.28, 95% CI 1.59–3.29).
Having any illicit substance use substantially increased the odds of having a NFOD (OR: 5.86, 95% CI 3.58–9.58). Records of cannabis (OR: 1.77, 95% CI 1.11–2.83), cocaine (OR: 2.35 95% CI 1.60–3.47), heroin (OR: 2.14, 95% CI 1.48–3.12), opioids not specified (OR: 2.19 95% CI 1.47–3.26) and synthetic cannabinoids (OR: 1.74, 95% CI 1.01–2.99) were positively associated with NFOs.
In general, physical or mental health conditions increased the risk of an NFO, including the presence of a respiratory condition (OR: 1.84, 95% CI 1.20–2.81), particularly asthma (OR: 1.96, 95% CI 1.26–3.04), or a blood-borne virus (OR: 2.19, 95% CI 1.46–3.28) or known migraines (OR: 2.21, 95% CI 1.06–4.62). Further risks included having diagnosed anxiety (OR: 2.27, 95% CI 1.59–3.26), depression (OR: 1.79, 95% CI 1.26–2.55), ADHD (OR: 3.12, 95% CI 1.14–8.52) or a personality disorder (OR: 4.92, 95% CI 2.96–8.17).
留言 (0)