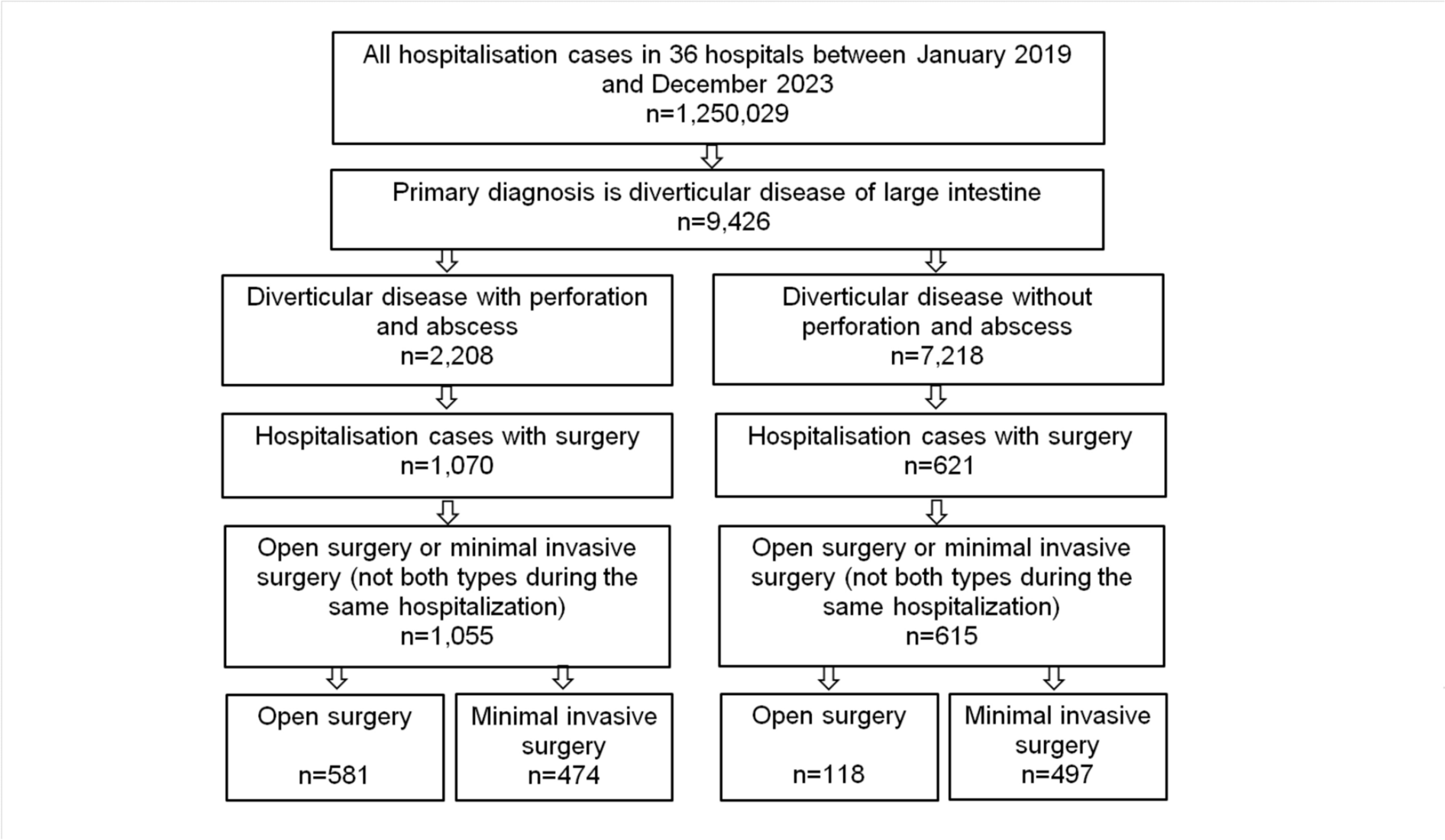
In this multicenter cross-sectional study, we analyzed the situation regarding the approach for surgical resection of colonic diverticular disease between 2019 and 2023 in a large patient cohort of 1670 patients from 36 German hospitals. Interestingly, our findings indicate that open surgery was the most commonly used approach for complicated diverticular disease presenting with perforation or abscess during this observation period. In addition, a trend of conventional procedures declining from 65.4% to 47.1% over this 5-year period became evident. Most importantly, since Curfman et al. [22] also reported a relatively high number of conventional open surgeries of almost 77% in a total of 2524 patients with perforated colonic diverticular disease between 2018 and 2021, our observation of a high percentage of open surgeries is internationally comparable. In an earlier registry study, Lee et al. found that, of 3756 patients with an indication for emergency sigmoidectomy for perforated colonic diverticular disease, 282 were performed completely laparoscopically, a rate of only 7.5%, which is even lower than our observed rate [20].
On the other hand, our study reveals a remarkable decrease in the proportion of conventional surgery performed for uncomplicated colonic diverticular disease, i.e., in patients who typically undergo elective surgery. Specifically, the rate of primary open resections of the colon decreased from 32.2% to 13.8% during the study period. Data from a recently published study by Ebrahimian and coworkers [23] using a US national readmission database (NRD) for the years 2017–2019 suggest that such rates are even higher in other countries. They found that 39.3% of 110,281 patients who were admitted for electively planned colectomy for diverticulitis underwent primarily open surgery, only 53.3% had completed laparoscopy, and 7.4% were converted to an open approach. At this point, however, we would like to emphasize that, to our knowledge, no study to date has presented such a detailed time course of the different surgical approaches for colonic diverticular disease.
In line with previous publications, we also observed a significantly lower morbidity rate in our study cohort when using a minimally invasive approach for both perforated and nonperforated colonic diverticular disease [20, 24]. Thus, the results of multivariate logistic regression analysis in our study cohort demonstrated that acute postoperative bleeding, respiratory failure, and other complications of the gastrointestinal tract were significantly more common with open surgery. In addition, hospital stay was significantly longer with open surgery.
The benefits of a minimally invasive procedure have been well described for elective surgery for diverticulitis [25,26,27,28]. Interestingly, there have been recent reports that suggest that the laparoscopic approach may also be a safe alternative for emergency surgery in cases of complicated diverticulitis [29, 30]. The study by Lee et al. [20] comparing laparoscopic and open sigmoidectomy for perforated diverticulitis using 3756 cases from the ACS-NSQIP database reported significantly lower complication rates, fewer unplanned intubations, and less acute renal failure in the minimally invasive group. Operative time was longer in the laparoscopic group, but hospital stay was shorter. In addition, a subgroup analysis comparing laparoscopic and open Hartmann’s technique and primary anastomosis with and without stoma diversion also demonstrated an advantage for the laparoscopically resected patients. However, it is important to note that there are no RCTs comparing minimally invasive surgery versus open surgery for perforated diverticulitis. Furthermore, the data from the large retrospective cohort studies suffer from significant selection bias. For example, these studies lack important information about the initial health status of the patients, such as the inability to create a capnoperitoneum for cardiovascular or respiratory reasons, which inevitably leads to uncontrolled high risk for patients in the open surgery group. This in turn fosters the risk that these patients may have worse postoperative outcomes and longer hospital stays.
An interesting observation was that, in both groups of diverticular disease, with and without abscess or perforation, more patients with defined secondary diagnoses underwent open surgery. In addition, the proportion of patients older than 70 years of age was higher in the group of patients who underwent conventional open surgery. A correlation between the comorbidities we observed and the surgical approach has already been described in the literature and is therefore consistent with our observations [23].
Thus, our results suggest that the choice of surgical procedure is strongly influenced by secondary diagnoses and age. Although we did not determine a comorbidity index in our cohort, it can be assumed that multimorbid patients and elderly patients are more likely to undergo conventional open surgery in Germany. Elderly patients are known to have higher rates of preoperative comorbidities and higher American Society of Anesthesiologists (ASA) scores than younger patients [31]. They also have a worse preoperative general condition than younger patients. In addition, laparoscopic procedures performed under capnoperitoneum and Trendelenburg positioning have been described to have negative hemodynamic and pulmonary effects, such as higher systemic vascular resistance, decreased ejection fraction, and impaired respiratory compliance [32]. Because of these concerns, laparoscopy is still often not considered in older patients and those with serious comorbidities, and our observations may reflect exactly this issue. However, it should be noted that the study by Braschi et al. [33], who analyzed patients older than 65 years of age from the ACS-NSQIP database, demonstrated that older patients who underwent both elective and nonelective laparoscopic procedures for diverticulitis had lower 30-day morbidity, fewer procedural complications, and shorter hospital stays than patients who underwent an open approach.
Another point that needs to be emphasized in this context is that the severity of disease may also influence the choice of surgical approach, especially for procedures performed owing to perforation or abscess. Therefore, it can be assumed that patients with severe sepsis are more likely to undergo open surgery for perforated colonic diverticular disease to save time and to be transferred more quickly to the intensive care unit for further treatment.
The second aspect to consider, which may also have influenced the number of open or minimally invasive resections in our study, is the surgical experience of the responsible surgeon, about which we unfortunately have no information. For example, at least 50 [34], and preferably 85 [35], laparoscopic colon resections are necessary to complete the learning curve and thus be able to perform technically demanding resections, such as those expected in acute perforated colonic diverticular disease, completely laparoscopically. Often, the most experienced surgeons are not always available outside of regular working hours and on weekends, when emergency procedures for perforated diverticulitis are most common, so an open approach is more likely to be chosen in the absence of expertise in minimally invasive colon surgery. The study by Ebrahimian et al. [23] also shows that the risk-adjusted conversion rate for laparoscopic sigmoid resections is directly proportional to the number of minimally invasive procedures performed at a hospital. Therefore, to increase the patient benefit of minimally invasive surgery, even in emergency situations, it is necessary to educate surgeons so that this advantageous surgical approach can be offered at all times. However, the observed increase in the number of laparoscopic procedures performed in our study may be indicative of a general trend toward increasingly sophisticated surgical expertise and manual skills for minimally invasive procedures.
Robotic surgery represents a novel approach to minimally invasive surgery. There has been a remarkable increase in the utilization of this technique in recent years, especially in the field of visceral surgery [36]. In the present study, a total of 971 minimally invasive colon resections were performed, with only 49 cases performed using a surgical robot. This represents a proportion of approximately 5% over the 5-year period. However, this result is consistent with the findings of Curfman et al. [22], who reported a rate of 5% in the context of emergency procedures. In this context, it should be mentioned that a systematic review suggests that the use of a robot for emergency procedures in general surgery is feasible [37]. Traditionally, a surgical robot is used for complex procedures, such as oncologic surgery, that are performed as part of a planned routine program. In addition, special training is required not only for the surgeons, but also for the nursing staff in the operating room to ensure efficient use. Thus, the use of a surgical robot outside of regular working hours for emergencies remains difficult to realize until comprehensive training of all staff has been completed.
It is important to be aware of the limitations of our study, even though a large cohort of patients was included. First, while this is a multicenter study using 36 hospitals, these hospitals represent only a small fraction of the roughly 2000 hospitals in Germany. Second, in our cohort it is not possible to estimate the number of emergency operations, which may have influenced the surgical approach, although this may have played a lesser role in the group of nonperforated cases and patients without abscess. The fraction of patients who underwent conventional open surgery may therefore have been in poorer general health, which may have contributed to higher complication rates, mortality, and length of hospital stay. In addition, it is unclear how many of the included hospitals had a robotic system and what the frequency of surgeries and surgeon experience were per hospital.
Taken together, our nationwide study reveals a significant shift toward minimally invasive surgery for colonic diverticular disease in Germany, reflecting its benefits in reducing in-hospital mortality, complications, and length of hospital stay. However, open surgery may predominate in complicated cases and perhaps owing to patient age and comorbidities.






留言 (0)