
記住我




NHANES, an ongoing series of nationally representative surveys conducted biennially, is dedicated to monitoring the nutritional and health status of the non-institutionalized US civilian population. Utilizing a sophisticated probability multi-stage sampling design, NHANES ensures the accuracy of estimates. Due to the COVID-19 pandemic, survey operations were halted in March 2020. Consequently, data collected from 2019 to March 2020 was merged with that from the 2017–2018 cycle, yielding the NHANES 2017–2020 pre-pandemic dataset. Ethics Review Committee of the National Center for Health Statistics approved the original survey protocol, and written informed consent was obtained from all participants. Given the use of publicly available and de-identified NHANES datasets, the current analysis does not necessitate the approval and informed consent of the Institutional Review Board. This study follows the reporting guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) [31].
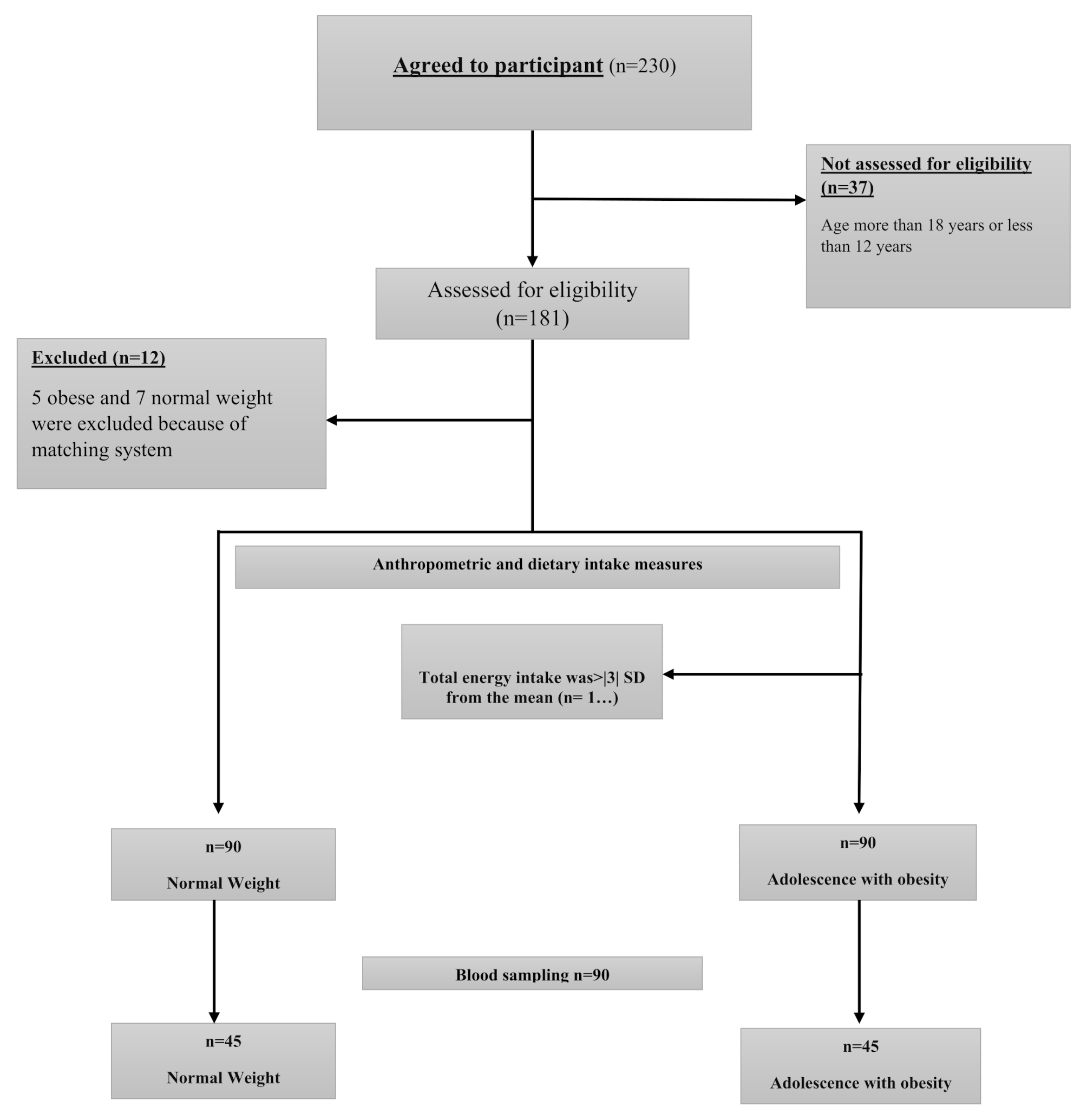
We opted for the NHANES cycle from 2017 to March 2020 due to its exclusive availability of data on liver ultrasound vibration-controlled transient elastography (VCTE). The detailed study flowchart is depicted in Fig. 1. Among the initial 15 560 participants, we excluded individuals based on the following criteria: (1) under 20 years old (n = 6328), (2) missing controlled attenuation parameter (CAP) values from hepatic VCTE assessments (n = 689), (3) ineligible (n = 333), not done (n = 222), or partial (n = 593) VCTE examinations, (4) excessive alcohol consumption, defined as more than three standard alcoholic drinks daily for males or two for females (n = 224), (5) missing data on CVH metrics (n = 1418), and (6) missing partial covariates data (n = 73), which included 58 missing aspartate aminotransferase (AST) values, 8 on thyroid disease history, 5 on education levels, and 2 on marital status. Ultimately, 5680 participants were included in the final analysis.
Fig. 1
Flowchart of participant selection. NHANES, National Health and Nutrition Examination Survey; VCTE, vibration controlled transient elastography; CAP, controlled attenuation parameter; CVH, cardiovascular health; AST, aspartate aminotransferase; MASLD, metabolic dysfunction-associated steatotic liver disease
Assessment of CVHLE8 score was applied to assess CVH, comprising four health behaviors (diet, physical activity, nicotine exposure, and sleep) as well as 4 health factors (BMI, blood pressure, blood glucose, and non-high-density lipoprotein [non-HDL] cholesterol) [23, 24]. Health behaviors scores were derived from questionnaire responses. Diet indicators were assessed using the Healthy Eating Index (HEI) 2015 [32], and its scoring criteria were showed in Supplementary Table S1. BMI and blood pressure scores originated from physical examination measurements, and blood glucose and non-HDL scores were based on laboratory analyses of blood samples. The method for computing LE8 score was documented in previous literature, with details provided in Supplementary Table S2. By averaging the scores of the 8 metrics, the overall CVH score was calculated. Similarly, scores for health behaviors and health factors were determined using relevant metrics. Scores ranged from 0 to 100, with higher scores indicating better health. In accordance with the guidelines set forth by the AHA, overall CVH, healthy behaviors, and health factors were classified into three categories: low (0–49 points), moderate (50–79 points), and high (80–100 points).
Definition of MASLDThe Fibro Scan® model 502 V2 Touch device was utilized for VCTE examinations at the mobile examination center to evaluate the CAP values and liver stiffness. An examination was considered complete if the fasting time was at least 3 h, there were 10 or more valid stiffness measurements, and the interquartile range/median of liver stiffness was 30% or less. We identified hepatic steatosis using a median CAP of at least 285 dB/m based on previous studies (80% sensitivity and 77% specificity for detecting 5% steatosis) [33, 34]. MASLD was defined as the presence of hepatic steatosis, at least one of the five cardiometabolic risk factors as recommended in the recent consensus statement [1], and the absence of excessive alcohol consumption (≥ 2 drinks for women and ≥ 3 drinks for men).
Assessment of covariatesCovariates in this study included age, gender (male/female), race/ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black, and other), education level (high school or less, some college or associates degree, and college graduate or above), marital status (married/living with partner, widowed/divorced/separated, and never married), poverty income ratio (PIR), alanine aminotransferase (ALT), AST, gamma-glutamyl transferase (GGT), obesity (yes/no), history of thyroid disease (yes/no), and sleep apnea (yes/no). Obesity was defined as BMI ≥ 30 kg/m2 [35]. Recent research has indicated a correlation between obstructive sleep apnea and the occurrence and progression of NAFLD [36]. Considering the widespread prevalence of sleep apnea in CVD patients and the significant role of sleep health in CVH assessment [23, 37], this study included sleep apnea as a covariate. The diagnosis of sleep apnea was based on the sleep questionnaire SLQ040 “In the past 12 months, how often did you snort, gasp, or stop breathing while you were asleep?”. The presence of sleep apnea was considered when the responses were rarely (1–2 nights per week), occasionally (3–4 nights per week), or frequently (5 or more nights per week).
Statistical analysisTo ensure the representativeness of the entire nation, this study considered the intricate sampling design of NHANES by utilizing sample weights in all analyses. Continuous variables were reported as weighted means and standard errors (SE), while categorical variables were presented as weighted percentages along with their respective 95% confidence intervals (CIs). Baseline characteristics of study participants were compared using unadjusted linear regression for continuous variables and Rao-Scott chi-square tests for categorical variables. Additionally, we calculated the age-standardized prevalence estimates and their corresponding 95% CIs for each CVH category.
Weighted binary logistic regressions were utilized to calculate the odds ratio (OR) and 95% CI to investigate the associations of CVH using the LE8 score with MASLD. Our study applied three models. Model 1 did not adjust for any potential confounders. Model 2 made adjustments for age, gender, and race/ethnicity. Model 3 further adjusted for education level, marital status, PIR, ALT, AST, GGT, obesity, history of thyroid disease and sleep apnea.
Restricted cubic spline (RCS) analysis with 3 knots (at the 5th, 50th, and 95th percentiles) was conducted to explore the nonlinear relationships between LE8 and its subscale scores with MASLD after adjusting for variables in model 3. The likelihood ratio test was utilized to evaluate nonlinearity. Subsequently, subgroup and interaction analyses were carried out based on gender, age strata (20–39 years, 40–59 years, and ≥ 60 years), race/ethnicity, education level, marital status, PIR (low income: PIR < 1.30, middle income: PIR ≥ 1.30, < 3.50, and high income: PIR ≥ 3.50), and obesity.
We also undertook three sensitivity analyses to confirm the robustness of our results. Firstly, we reanalyzed the data by excluding participants who self-reported a history of CVD, encompassing heart attack, angina, coronary heart disease, or stroke (n = 559). Secondly, we employed multivariate multiple imputation with chained equations to impute missing values. Missing data for both sleep apnea and PIR were imputed. Finally, repeated analysis was conducted by using a median CAP value of 263dB/m or more as the definition of hepatic steatosis (90% sensitivity) [38]. All statistical analyses were conducted using R version 4.2.1 software (R Foundation for Statistical Computing, Vienna, Austria). A 2-sided P-value less than 0.05 was deemed statistically significant.
留言 (0)