AL-CA is a relatively rare disease that poses diagnostic challenges. Not all medical institutions are equipped to perform comprehensive haemodynamic assessments, making research on the haemodynamics of patients with AL-CA relatively rare. Our study specifically targeted patients with stage IIIb disease and revealed that their haemodynamics are characterized by a significant increase in biventricular filling pressure, whereas stroke volume and CI only slightly decrease.
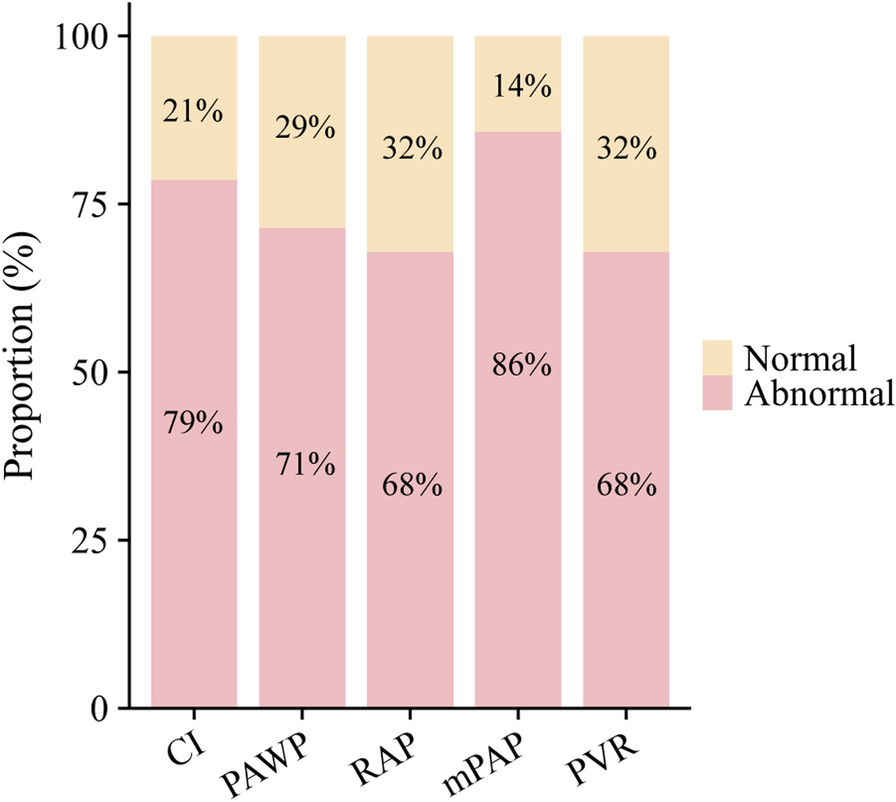
The majority of patients included in our study were elderly or middle-aged males, which is consistent with the known demographic characteristics of this disease. Nearly all patients presented with significant heart failure symptoms. The markedly elevated levels of NT-proBNP and cTnI indicate severe cardiac injury in stage IIIb patients, with almost half of the patients also experiencing renal dysfunction, likely due to the combined effects of light-chain amyloidosis and impaired cardiac function. Additionally, the average time from symptom onset to diagnosis was nearly one year, suggesting a heavy disease burden for these patients and highlighting the ongoing challenges in diagnosing this condition. Echocardiography revealed that most patients still presented with an HFpEF pattern, with significantly impaired diastolic function and notably thickened ventricular walls, indicating that even in stage IIIb patients, a decrease in LVEF is relatively uncommon. However, haemodynamic data obtained through RHC revealed a significant reduction in CI for most patients, along with elevated PAWP, mPAP, and PVR, suggesting that both systolic and diastolic functions are notably compromised in stage IIIb patients.
Even though daratumumab has optimized the proportion and rate at which patients with AL-CA achieve a cardiac response, the early mortality rate among stage IIIb patients remains high at 22.8% [14]. In our cohort, all deaths were early deaths, whereas survivors responded exceptionally well to treatment without experiencing worsening heart failure or other adverse events. Therefore, identifying factors contributing to poor outcomes in stage IIIb patients can help clinicians identify those who fail to benefit from treatment early. Prior research has investigated how haemodynamic measurements can predict outcomes for patients suffering from AL-CA. The focus was on assessing whether these indicators could serve as reliable predictors for patient prognostics. A study published in 2013 involving 89 AL-CA patients identified the RAP as a primary predictor of free-heart transplantation survival [15]. In 2023, an extensive study including 198 individuals diagnosed with AL-CA demonstrated the substantial prognostic value of CI in forecasting outcomes such as all-cause mortality, the need for heart transplants, and the use of left ventricular assist devices more than other haemodynamic parameters. Although the PAWP is significantly elevated, it is not independently associated with prognosis [13]. In summary, the CI, which reflects systolic function, and the PAWP, RAP, mPAP, and PVR, which reflect diastolic function, are considered potentially associated with prognosis. However, the results from different cohort studies vary, likely due to the dynamic nature of patients' haemodynamic status, and a single baseline measurement may not provide enough information. This study focused on examining the role of haemodynamic data in patients with stage IIIb disease, as these patients are critically ill and require haemodynamic guidance in the intensive care unit. Additionally, we aimed to assess whether these data can be used to evaluate long-term prognosis in such patients. In our stage IIIb AL-CA cohort, we incorporated key haemodynamic parameters into the survival analysis, which yielded no meaningful results. We also discovered that the cardiac injury biomarkers NT-proBNP and cTnI were not associated with prognosis. Similarly, the eGFR, an indicator of renal function impairment, was not statistically significant according to the Cox regression model. Innovatively, we propose the PAWP/CI ratio as a new parameter. Compared with other conventional haemodynamic parameters, the PAWP/CI ratio better reflects the condition of patients whose PAWP is significantly elevated even when there is only a mild decrease in CI, thereby accentuating the extent of cardiac output impairment and diastolic dysfunction. The results of our investigation revealed an independent correlation between the newly identified PAWP/CI ratio and all-cause mortality among stage IIIb AL-CA patients. This study also identified a clear cut-off value for PAWP/CI, which demonstrated excellent predictive performance for 6-month all-cause mortality in AL-CA stage IIIb patients. Given the extremely short median survival and high early mortality rate in stage IIIb patients, this parameter and its cut-off value can be highly valuable in clinical practice. It can assist clinicians in more accurately assessing patient prognosis and adjusting treatment strategies in a timely manner.
Our research supports the implementation of haemodynamic measurements in all patients with stage IIIb AL-CA to better assess their prognostic outcomes. However, a significant number of medical institutions are unable to standardize the use of RHC, or some patients' financial situations do not support such procedures. Given that nearly all patients with cardiomyopathy undergo echocardiography and that the literature indicates that, in certain cases, echocardiography can partially substitute for RHC [16, 17], we further explored echocardiographic parameters that could replace the PAWP/CI ratio. Our findings indicate a direct association between elevated PASP and an increase in the PAWP/CI ratio, rather than LVEF or other indicators of cardiac structural abnormalities. PASP is calculated by experienced cardiologists via the measured tricuspid regurgitation velocity combined with an estimated RAP. Previous studies have shown a positive correlation between PASP measured by echocardiography and sPAP measured by RHC [18]. Additionally, the PASP has been found to predict the risk of sudden death in patients with pulmonary hypertension [18], suggesting that the PASP can, to some extent, serve as a noninvasive substitute for invasive haemodynamic measurements. These findings further suggest that diastolic dysfunction, not systolic dysfunction, leads to worse cardiac function and prognosis in patients with stage IIIb AL-CA. Although our results indicate that the MLVWT and LVMI are not linked to an increase in the PAWP/CI ratio, we believe that the ventricular wall abnormalities caused by amyloid deposition are related to haemodynamic abnormalities. We hypothesize that the lack of statistically significant results may be due to the inability of echocardiography to accurately measure cardiac amyloid deposition.
There are many clinical implications of our findings. First, the identification of a specific haemodynamic cut-off provides a tangible parameter for clinicians to target therapeutic interventions, potentially guiding treatment adjustments and monitoring strategies. Second, our research highlights the need for a fundamental change in handling stage IIIb AL-CA, suggesting a more haemodynamically informed approach that goes beyond conventional cardiac imaging and biomarker assessment. Finally, in the absence of haemodynamic results, echocardiography may serve as a potential alternative to RHC to some extent.
However, our study is not without limitations. The retrospective nature of the analysis, while comprehensive, is inherently subject to biases associated with historical data collection and patient selection. One of the other limitations is the restricted sample size, which inherently affects the generalizability of our findings. While we have endeavoured to ensure the robustness and validity of our analysis through rigorous statistical methods, the relatively small cohort may not fully represent the broader population. This limitation is particularly relevant when considering the heterogeneity of the conditions under investigation, where individual variations could significantly influence outcomes. Therefore, it is important to interpret our findings carefully, as broader and more varied samples could lead to different conclusions.






留言 (0)