
記住我






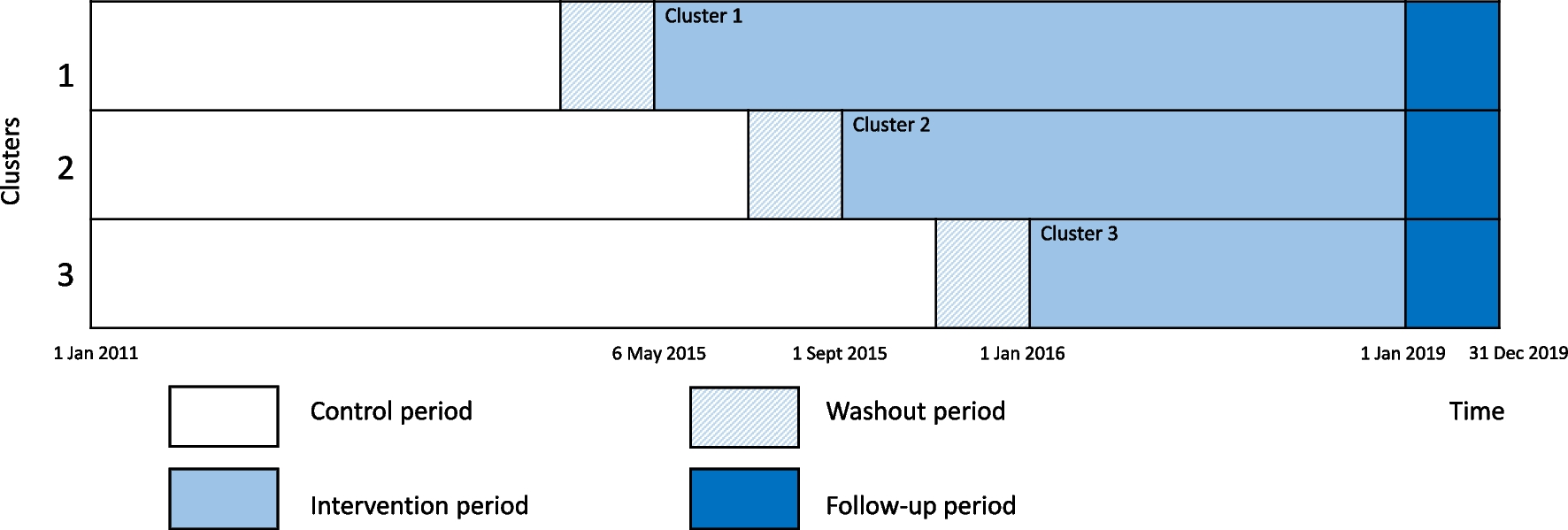
The Norwegian Capture the Fracture Initiative (NoFRACT) study was designed as a pragmatic, multicenter, register-supported, stepped-wedge cluster-randomized trial (SW-CRT). The stepped-wedge design was chosen to ensure that all study sites received the intervention during the study period. Further, the prospective SW-CRT design allowed for both a randomized trial design and to take time trends in fracture rates into consideration. The study was registered (Clinicaltrials.gov, NCT02536898) and the trial protocol has been published [22]. Seven Norwegian hospitals were randomized for the order of starting date, and divided into three clusters, with an interval of 4 months between the clusters (Fig. 1). Randomization was performed by the Norwegian Osteoporosis Association, who had no other involvement in the study. Standard care was delivered at each hospital during the control period (2011–2015) and the hospitals crossed over in only one direction and delivered the standardized FLS during the intervention period (2015–2018). The intervention was not blinded. The Consolidated Standards of Reporting Trials reporting guideline (CONSORT) with extension for SW-CRTs was followed for this trial. This is the first major report from the NoFRACT study.
Fig. 1
Study design of the NoFRACT intervention as recommended by the Consolidated Standards of Reporting Trials (CONSORT) extension for stepped-wedged cluster randomized trials (SW-CRTs)
Study interventionThe control period started on 1 January 2011 and went on until the stepwise introduction of the FLS intervention at each cluster. The FLS intervention was carried out at departments of orthopedic surgery at the NoFRACT hospitals with recruitment from 6 May 2015 until 31 December 2018 and follow-up through December 2019 (Fig. 1). All women and men ≥ 50 years with low-energy fractures (except fractures of the fingers, toes, face, and skull) who were treated at one of the NoFRACT hospitals and residing within each hospital’s catchment area were eligible for the FLS intervention. Exclusion criteria were short life expectancy judged by the treating physician.
The fracture patients were identified by a coordinating nurse and offered information, clinical assessment, lifestyle advice, and AOD if indicated, while they were in the hospital for their index fracture or as out-patients [22]. Lifestyle advice about physical activity, fall prevention, healthy diet, smoking cessation, and moderate alcohol intake was given, and referral to fall prevention at the hospital or primary care if indicated. The fracture risk assessment included BMD measurements using dual-energy X-ray absorptiometry (DXA) of both hips and spine, and/or calculation of the 10-year probability of a major osteoporotic fracture (MOF) using the Fracture Risk Assessment Tool (FRAX), and serum analyses of 25-hydroxyvitamin D, calcium, parathyroid hormone, thyroid-stimulating hormone, albumin, and creatinine to assess secondary causes of osteoporosis and the kidney function. AOD was offered directly to patients with a hip fracture, a vertebral fracture, or two or more low-energy fractures while they were still in the hospital, without the need of BMD or FRAX score assessment. Patients with a low-energy fracture of any other type were offered assessment within 6 weeks after their index fracture and treatment with AOD if BMD T-score ≤ − 1.5 or FRAX score for MOF > 20%. The primary drug of choice for patients with a hip fracture was intravenous zoledronic acid administered during the hospitalization for surgery. For patients with their first low-energy fracture, other than hip fracture, oral bisphosphonate, preferentially alendronate once weekly, was the drug of choice. Denosumab was an option in case of reduced kidney function (estimated glomerular filtration rate (eGFR) 20–35 mL/min). Patients with BMD T-score ≤ − 3.5, or subsequent low-energy fracture while on anti-resorptive treatment, were referred to an osteoporosis specialist to consider osteoanabolic treatment [22].
Audit data from each hospitalAudit data from the fracture patients during the NoFRACT intervention period was collected at each hospital. Aggregated summaries of the registration were used to monitor the number and proportion of patients who were offered FLS, had their fracture risk assessed, and were prescribed AOD. The ethical clearance for the collection of such data was given for local surveillance only and could not be linked to the register data.
Administrative register data from the Norwegian Patient Register (NPR)The main analyses were based on data retrieved from NPR after the end of the intervention period, on all women and men ≥ 50 years at the time of index fracture (2011–2018), who were treated at a NoFRACT hospital. An 11-digit person identification number enabled the merging of data to other data sources and the identification of index and subsequent fractures in the data. NPR also provided data on age, sex, and Charlson Comorbidity Index (CCI) based on registered diagnoses within the same year as the fracture [23]. However, the data from the NPR did not include information on whether the patients were exposed to the FLS intervention and had a BMD scan or AOD prescribed. We had no registered data on participation in the FLS intervention, and patients were placed in the control or intervention period solely based on the time of index fracture. Therefore, the analysis was an intention-to-treat analysis. As described above, we have included some aggregated audit data from the hospitals to help in interpreting the effect of FLS.
Statistics Norway provided data for all patients: dates of migration and death, marital status (never married, previously married, and married), country of birth (Scandinavian (Norway, Sweden, and Denmark), and non-Scandinavian), municipality of residence at time of fracture. Statistics Norway also provided an urban centrality index for each municipality: a score from 1 (most central) to 6 (least central) based on the number of inhabitants and the driving time from residential housing to jobs and services [24].
Outcome measuresAs registered in www.clinicaltrials.gov, the primary outcome was the change in the rate of subsequent fragility fracture defined as a fracture of the distal forearm, proximal humerus, and/or hip in patients with any type of index fracture. The secondary outcome was all-cause mortality in patients with any type of index fracture.
Additional outcomes were the change in the rate of any type of subsequent fracture, subsequent hip fracture after any type of index fracture, and second hip fracture and mortality after an index hip fracture.
Patients who were registered with a code for fracture control (International Classification of Diseases version 10 (ICD-10) Z-codes), fracture follow-up treatment (ICD-10 T-codes), and/or a Nordic Medico-Statistical Committee (NOMESCO) surgical procedure codes (NCSP) for reoperation were excluded from the analysis. Hip fracture diagnoses in the NPR have previously been validated [25]. The combined Cohen’s kappa for comparison of register data with fractures in local fracture registries was 0.95. We have also performed a study investigating forearm fracture validity in administrative hospital data using X-rays and/or medical records for verification [26]. The sensitivity (completeness) of the forearm fracture registrations was 90%. The positive predictive value increased from 74% in crude data to 91% when using a washout period of 6 months, and consequently, we applied a 6-month wash-out within each fracture group (ICD-10 S-code). Additionally, as fracture location can be miscoded, a 30 day-washout between registrations of fracture of the arm (S42, S52, and S62); ribs, spine, and pelvis (S22 and S32); and leg and foot (S82 and S92) were applied.
Statistical analysesAll results are presented for women and men separately. We used stratified Cox proportional hazard regression analysis to calculate hazard ratios (HRs) with 95% confidence intervals (CIs). The stratified Cox models allowed hospitals to act as their own control with individual baseline hazard functions. An index fracture was defined as the first fracture after a fracture-free wash-out period of 3 years. The 3-year wash-out period led to the possibility that some patients could count in both the control and intervention periods; therefore, repeated measures by individuals were additionally accounted for in the stratified Cox model. Follow-up measures for fracture outcomes were years contributed by each patient from the date of the index fracture to the first subsequent fracture, death, migration, or end of follow-up on December 31, 2019, with a maximum follow-up of 4.7 years. The follow-up measure for mortality outcome was years contributed by each patient from the date of the index fracture to death, migration, or end of follow-up on December 31, 2019, with a maximum follow-up of 4.7 years. In the analyses of mortality, patients could contribute with person-time in multiple episodes if they sustained subsequent fractures before they died. The stratified Cox model ensured equal maximum follow-up time in the control and intervention period, which was a requirement for using this method. The proportionality of the HRs was verified using log–log plot of survival by intervention status, adjusting for age, sex, hospital, and time.
The following regression analyses were performed for the primary and secondary outcomes as registered in www.clinicaltrials.gov: (a) from any type of index fracture to a subsequent fragility fracture, (b) from any type of index fracture to death. Additional analyses were (c) from any type of index fracture to any type of subsequent fracture, (d) from any type of index fracture to a subsequent hip fracture, (e) from an index hip fracture to a second hip fracture, and (f) from an index hip fracture to death. (Definitions of type of fractures are shown in Table 1).
Table 1 Definitions of types of fracturesWe also performed a multiple failures analysis where data were organized as ordered episodes and all fracture episodes from 2011 to 2019 were included. Since it was not possible to distinguish index fractures from other fractures, we included data from 2019 in this analysis, and consequently, the total number of patients differed from the main analyses.
Confounders were mapped using a causal-directed acyclic graph [27]. We estimated crude HRs for the association with the FLS intervention and HRs after adjustment for age, sex, urban centrality index [24], marital status, education level, Scandinavian-born, Charlson Comorbidity Index [23], fracture number, and type of index fracture. To account for time trends (declining subsequent hip fracture rates during the last 20 years) [28] and time-dependent randomization in the SW-CRT design, the analyses were adjusted for the day of hospital admission of the index fracture (cubic spline with 7 knots). Stata 16 (StataCorp, College Station, TX, USA) was used for the analyses.
Deviations from the protocolThe University Hospital of North Norway introduced the intervention on 1 October 2015, which was 5 months later than scheduled. Haukeland University Hospital initiated treatment with zoledronic acid directly only in patients with hip fracture > 70 years of age. We intended to start FLS treatment within 6 weeks after an index fracture; however, due to delay in the assessment of fracture risk, osteoporosis treatment may have been initiated after more than 6 weeks in some patients. As stated in the protocol article, we planned to exclude patients outside the hospitals’ referral region [22]; however, it was not possible to obtain hospital-specific data from The University Hospital of North Norway and Oslo University Hospital for the entire period, and data from the entire health trusts therefore had to be used. A multilevel regression model, where individuals count only once, was described in the protocol article [22]. However, SW-CRT was a relatively new study design when we planned NoFRACT. Statisticians who have experience with data analysis from a SW-CRT clearly recommend that the best way to accommodate cluster effects by hospital and individuals in our setting was to use a stratified Cox model including a term for repeated measures by individual (confer statistical analyses for more information). Using this method, patients in both the control period and intervention period had an equal chance to be included and have their fracture counted, when having a subsequent fracture within a similar 3-year period of washout. This is of importance to avoid variation in inclusion criteria as well as selection bias.
留言 (0)