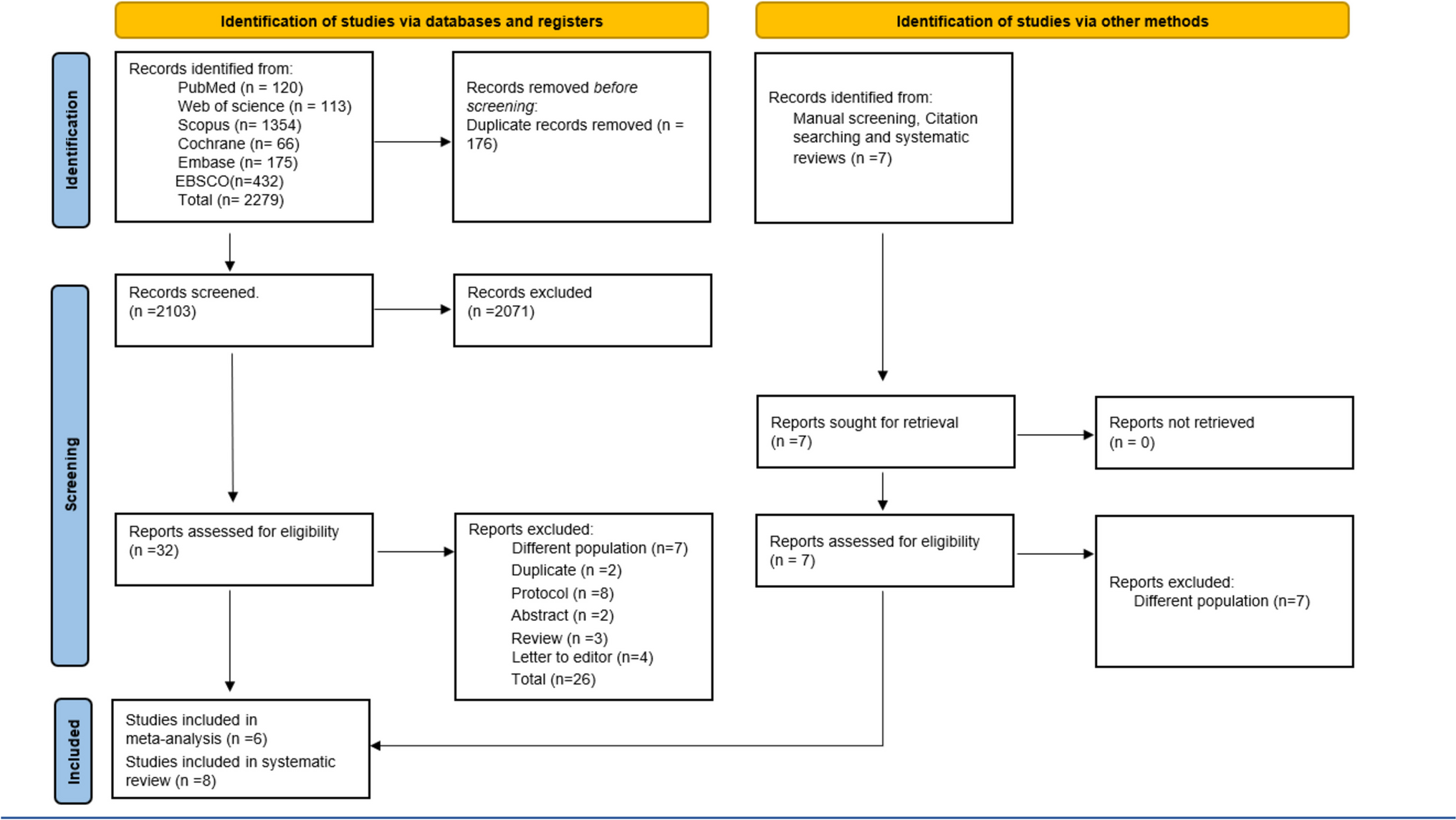
This study evaluated the compliance of UK-marketed complementary FIYC under 36 months with the NPPM. Of the 469 products assessed, 205 (45%) met the nutrient composition criteria, though none adhered to promotional requirements due to inappropriate claims on the labels.
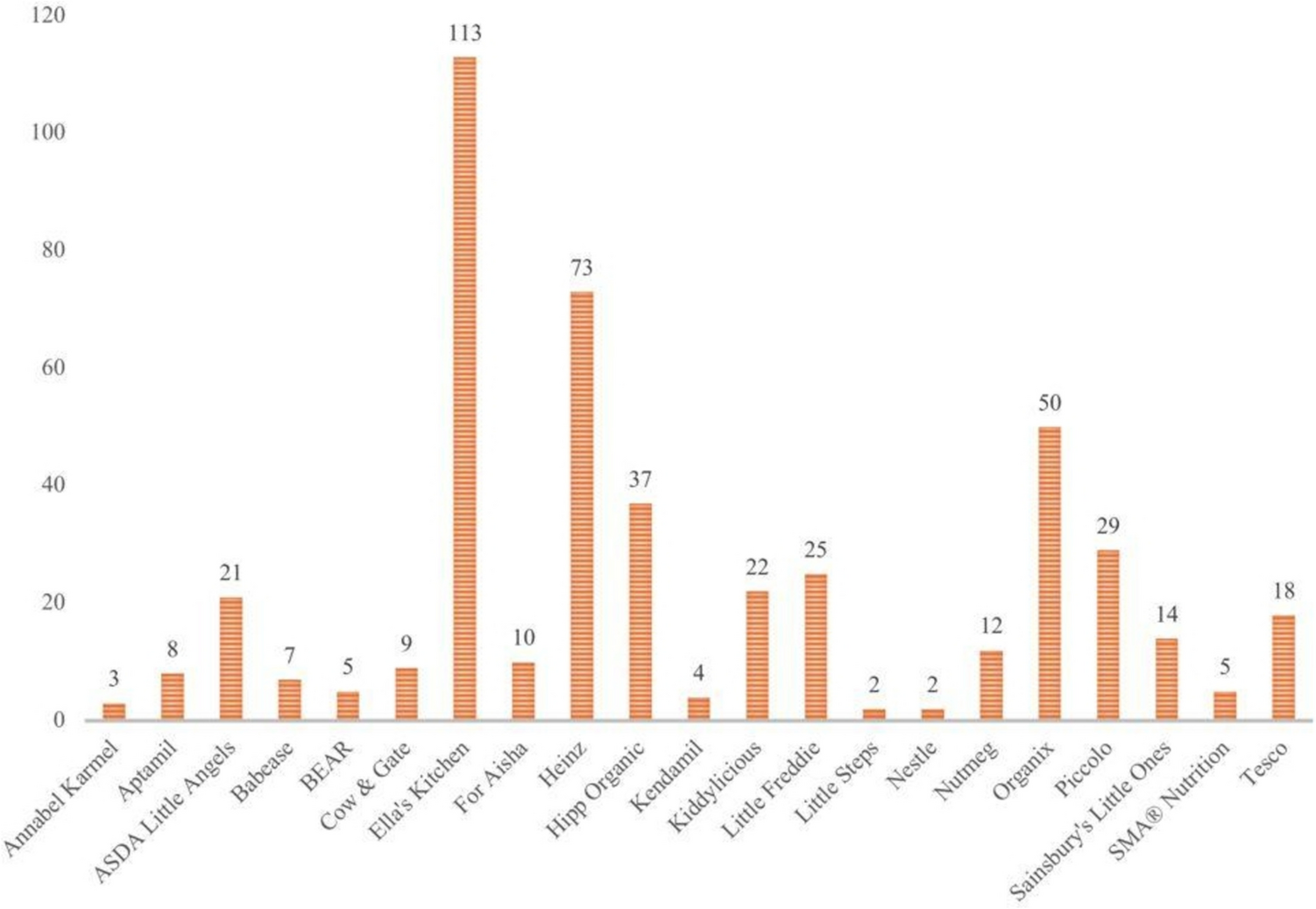
Product availability varies geographically and is typically linked to neighbourhoods [21]. In this study, similar to the results of the Public Health England report [16], the most common product type was meals, followed by fruit and vegetable purées/smoothies, fruit desserts, snacks, and finger foods. The most common FIYCs in other countries are fruit and vegetable purees in Poland [22], Portugal [23], and Russia [24]; cereals in Turkey [25] and Indonesia; ready-to-eat finger foods and snacks in Cambodia; and pureed foods and meals in the Philippines [26].
Energy density is a critical aspect for FIYC ensuring that foods are adequate for growth and development. Vegetable purées do not have a minimum energy density requirement as they often have a naturally high-water content [21]. Different flavours and vegetables should still be offered during weaning (6 to 12 months). A maximum added water requirement is included for vegetable purées to ensure that they are not too low in energy. Fruit and vegetable purées were the product groups with the lowest energy density in this study, similar to Hutchinson et al. [27] and Santos et al. [23]. Low energy density can be a problem because babies’ and young children’s small stomachs limit their mealtime consumption [22]. The NPPM suggests a minimum energy density of at least 60 kcal/100 g for several product categories which represents a conservative benchmark against the energy density of breastmilk [15]. In the NPPM, dry cereals and starches must have a minimum energy density requirement of 80 kcal/ 100 g (as eaten) to ensure foods are more energy dense than milk and to align with existing EC requirements. Although most relevant products (75%) met the NPPM energy density levels, about half (40%) of the fruit purées and about a quarter (22%) of the meals were below the recommendations. In the NPPM pilot study, most products met the energy density standard (81% in the UK, 68% in Denmark, and 84% in Spain), although approximately half or less of the fruit purées and meals in the UK and Denmark met the energy recommendations [21].
Conversely, the consumption of snacks with high energy densities and low nutrient values can lead to excessive energy intake [28]. Snacks were the product category with the highest energy density in this study, and half (51%) of UK snacks exceeded the NPPM recommended energy per portion of 50 kcal (≤ 50 kcal per serving or portion) [15] compared to 72% in Turkey [25].
Most products did meet the protein requirements, similar to the results of the Polish study [22], except for some meals. High income countries, such as the UK with an already high protein intake even in early childhood the necessity of maintaining a high protein intake is nuanced. Whilst protein is essential for growth other nutrients from a range of food sources are also needed. Some FIYCs might have less protein than their homemade equivalents, resulting in an insufficient intake of essential nutrients [15, 29]. A high protein diet in infancy has been suggested as a risk factor for childhood overweight and obesity [30]. This raises the possibility of adding upper limits for protein to the NPPM.
Added sugars are widely used in various product categories, and a significant number of savoury meals contain pureed fruit, particularly in the UK [27]. According to the NPPM criteria, no products marketed for children under 36 months should contain added sugar [15]. However, this study found that 19% of products did contain added sugars. In a 27-country study by Grammatikaki et al., 39% of products contained sugar-added ingredients, with 10% listing added sugar, 14% free sugar, and 20% fruit purées and powders [31]. In the NPPM pilot study, 28% of UK, 21% of Danish, and 44% of Spanish products included added sugars [21]. Differences in sugar definitions and product types, such as the exclusion of sugars from vegetable purees, may account for these variations. Added sugars remain a concern, with NPPM defining them as monosaccharides and disaccharides added during processing, while free sugars include those naturally found in honey, syrups, and fruit concentrates. Liberated sugars, released during processing, also contribute to sweetness and rapid absorption [15].
In the new NPPM, the WHO has suggested that products with high sugar levels should not be marketed as appropriate for infants and young children. In addition, the NPPM recommends that products with more than 30% (cereals, fruit/vegetable purees), or 40% (dairy) calories from total sugars, should carry a front-of-pack flag on the label/packaging to indicate the presence of high sugar levels [15]. In this study, 46% of products exceeded FOP limits, and 41% surpassed total sugar thresholds. Nearly half of meals and one-third of snacks had excessive sugar (i.e., >15% of energy), with most fruit and vegetable purées exceeding 30% sugar content, making total sugar the most common cause of non-compliance. High sugar intake in infancy raises risks for dental caries and metabolic diseases [32].
Avoiding added salt in children’s foods is also crucial, as it affects taste preference and long-term health [33]. Although 86% of products met the salt limits, 22.5% of meal contained more salt than recommended. Compliance with sodium standards is higher in the US [34], New Zealand [35], and Portugal [23] but lower in Cambodia and Indonesia, where only one-third and half of the products, respectively, met the WHO NPM sodium standards [26]. Cambodia lacks sodium content standards for commercial FIYC products, while Indonesia’s sodium standard is more than twice the WHO NPM standard (50 mg/100 kcal) [26]. This highlights the role of compositional limits in managing nutrients of concern in commercial FIYC products.
In the draft NPPM applied across multiple countries, the percentage of items meeting all composition criteria ranged from 15% in Hungary to 42% in Estonia, with 31% of UK products meeting these criteria [21]. It should be noted that the draft NPPM differed slightly from the final version used here, as it did not include limits for dried or puréed fruit or energy density per serving for finger foods. In this study, 45% of UK products met the updated WHO NPPM criteria, compared to 29% in Turkey [25].
Promotion is considered inappropriate if it is misleading, confusing, or likely to lead to inappropriate use; for example, if it contains claims that idealize the products, compromise breastfeeding, or imply that they are better than family foods [36]. All products in this study displayed promotional claims on composition, nutrition, or health. Similarly, almost all products in four WHO European countries (95–100%) [37] and seven Southeast Asian countries (98.6%) [38], carried some type of statement on composition, nutrition, or health-related promotions.
The WHO recommends exclusive breastfeeding until six months, followed by continued breastfeeding alongside complementary foods up to two years or beyond. This guideline is also supported by UK public health authorities, which advise against introducing complementary foods before six months [40, 41]. Breastfeeding duration is shorter in high-income countries than those that are resource poor. Despite evidence of protection against childhood conditions and later life ill health for the mother. Breastfeeding up to two years and beyond supports the health and neurobiological development of an infant and a young child [40]. Although UK market surveys show a decrease in products marketed for infants under six months (from 43% in 2013 to 23% in 2019), the range of products targeting this age group has increased from 178 to 201 types [17]. In present study, 14% of products were still marketed as suitable for infants under six months, highlighting a need for regulatory action.
The high non-compliance rates, particularly regarding “claims and breastfeeding support,” highlight the need for stricter promotional regulations to avoid conflicts with public health messages and maintain caregivers’ trust in baby foods. This study found that only 45% of UK FIYC products met nutrient composition criteria, with high sugar content being the main area of non-compliance, and none met NPPM promotional standards. These findings underscore the importance of comprehensive labelling standards and regulatory updates to reduce misleading claims and added sugars, promoting healthier dietary patterns for infants and young children.
This study has several limitations. Firstly, it relied on product label information from supermarket websites, which did not always fully meet NPPM standards (e.g., fruit content, added water, protein, age recommendations). Additionally, the lack of data on the proportion of commercial versus home-prepared foods consumed by UK infants and young children may limit the generalisability of the findings. Secondly, the analysis relied on manufacturer-reported nutrient content rather than independent laboratory testing.





留言 (0)