
記住我
Diabetes mellitus is a chronic metabolic disease characterised by a disorder of glucose metabolism resulting from the consistent presence of beta-cell dysfunction leading to insufficient insulin secretion, reduced insulin sensitivity, or both. In 2021, there were 529 million(95% uncertainty interval [UI] 500-564) people with diabetes globally, with an overall global age-standardised prevalence of diabetes of 6-1%(5-8-6-5), and a global age-standardised prevalence of diabetes of 6-1%(5-8 -6-5), representing a major public health challenge (1).
In addition to the most common secondary complications of diabetes including diabetic retinopathy, nephropathy, neuropathy, and cardiovascular disease (2), bone disorders are frequently diagnosed, and thus diabetes is classified as a bone-related disease. It is characterised by altered bone mineral density(BMD), abnormal bone metabolism and microarchitecture, and reduced bone strength (3).
Recent studies have suggested that osteocalcin may play an important role in regulating blood glucose levels and controlling the development of diabetes mellitus (4). Osteocalcin, also known as bone γ-carboxyglutamic acid(Gla) protein or BGP, is a 46-50 amino acid, 5.6 kDa secreted protein produced mainly by osteoblasts (5), while osteocalcin(OC) is the most abundant non-collagenous and osteoblastic bone secreted protein. It consists of carboxylated OC(cOC) and undercarboxylated OC(ucOC) forms (6).
OC, especially ucOC, can improve pancreatic function and metabolic status by targeting multiple tissues essential for glucose and lipid metabolism. In the pancreas, ucOC can directly promote β-cell proliferation and insulin production via GPRC6A (7, 8), and ucOC also indirectly promotes insulin production by increasing intestinal glucagon-like peptide-1 (GLP-1) levels and thereby promoting GPRC6A secretion (9). In insulin-targeted tissues, ucOC can increase glucose and fatty acid uptake (10), insulin sensitivity (11), nutrient utilisation and mitochondrial capacity, and reduces glycogen production in muscle and lipid synthesis in the liver (12, 13). Moreover, non-carboxylated osteocalcin ucOC is regulated by insulin and increases β-cell proliferation as well as insulin production and secretion, whereas skeletal muscle and adipose tissue respond to osteocalcin by increasing insulin sensitivity (14).
The study of the link between osteocalcin and diabetes suggests that we can control blood glucose by regulating osteocalcin levels.
A substantial body of evidence from numerous studies indicates that osteocalcin plays a role in regulating insulin secretion and in the prevention and treatment of diabetes. The numerous cross-sectional studies conducted provide a strong scientific basis and practical application for this finding.
In a comprehensive and systematic review of previous studies on osteocalcin, Meredith L. Zoch (14) and colleagues provide a new perspective on the role of osteocalcin in bone metabolism, reproduction, and cognition. They demonstrate that osteocalcin is a bone-derived factor that affects these processes through endocrine circuits in bone. This study challenges the conventional view of osteocalcin perception.
Naomi Dirckx (15) and others further reviewed and analysed the research in this field in relation to osteoblasts, reviewing the specific response of osteoblasts to metabolic hormones as well as the production of at least three endocrine factors affecting whole-body metabolism from an osteoblast perspective. Setor Kwadzo Kunutsor (16) et al. reviewed and meta-analysed serum total osteocalcin in relation to type 2 diabetes and intermediate metabolic phenotypes. Dong-Mei Liu et al. (17) outlined bone as another potential target for the treatment, prevention and prediction of diabetes. Yixuan Li (18) et al. focused on bone-derived hormones such as fibroblast growth factor 23 and osteocalcin, and summarised their new therapeutic roles in the regulation of diabetes and diabetic nephropathy. Monika Martiniakova (3) and others discussed the current role of osteocalcin in the management and treatment of diabetes mellitus, osteoporosis, osteomalacia, and inflammatory joint diseases from a preclinical as well as a clinical research perspective, and reviewed the latest disease research advances of osteocalcin.
Although the above review articles provide insights and value for understanding some specific aspects of the research on the relationship between diabetes and osteocalcin, they fail to consider the skeleton as a whole as an endocrine organ. Instead, they focus on osteocalcin as part of the narrative, examining only the mechanism of osteocalcin or the treatment of diabetes. Furthermore, these reviews do not analyse osteocalcin and diabetes in a systematic manner. They also fail to provide insights into the range of topics covered in the research area, as well as the composition and geographical distribution of influential journals and distinguished authors and institutions in this scientific field, and its history and latest trends. Furthermore, the articles in question do not provide insights into the range of topics covered by the research area, nor do they offer an overview of the scientific field in terms of influential journals, the composition of distinguished authors and institutions, or the geographical distribution. They also fail to provide information on the history and recent trends of the field. This is not a deficiency of the literature itself, but rather a consequence of the choice of focus, coverage, and research methods and tools employed in these review articles.
Bibliometrics is a comprehensive scientific mapping and analysis tool that enables the analysis and processing of vast quantities of literature information, thereby enhancing the efficiency of scientific research (19). It is employed to illustrate relationships, such as citations, collaborations, and co-occurrences, within the literature. It is also used to construct various types of knowledge graphs and to explore the critical paths, research hotspots, and cutting-edge directions of the evolution of a discipline or field. The visualisation method of co-citation analysis in bibliometrics assists in the interpretation of data and defines a relationship between two articles if they are cited by one or more other articles at the same time. Co-citation analysis allows for the assessment of the relative importance placed by researchers on the cited literature.
However, to the best of our knowledge, there are no previous bibliometric studies that have reported an association between osteocalcin and diabetes.
It was therefore our intention to address this knowledge gap. In this study, the bibliometric software Bibliometrix and the visualisation tool VOSviewer were employed to analyse the literature pertaining to osteocalcin and diabetes and to map scientific knowledge.
Materials and methodsLiterature sources and search strategyAfter obtaining relevant title keywords from PubMed and supplementing them with web subject terms, we initiated an exhaustive online bibliographic search via WoS in the following format:
All articles from October 1986 to May 2024 were searched in the Web of Science Core Collection (WoSCC) database using the search formula (ALL = (Osteocalcin)) AND ALL = (diabetes or diabetes mellitus).
A meticulous examination of the extant literature yielded 1979 potential results, which were subjected to a rigorous screening process. This yielded the registration of 1680 papers, as illustrated in
Figure 1-Inclusion and exclusion criteria for diabetes in osteocalcin studies.
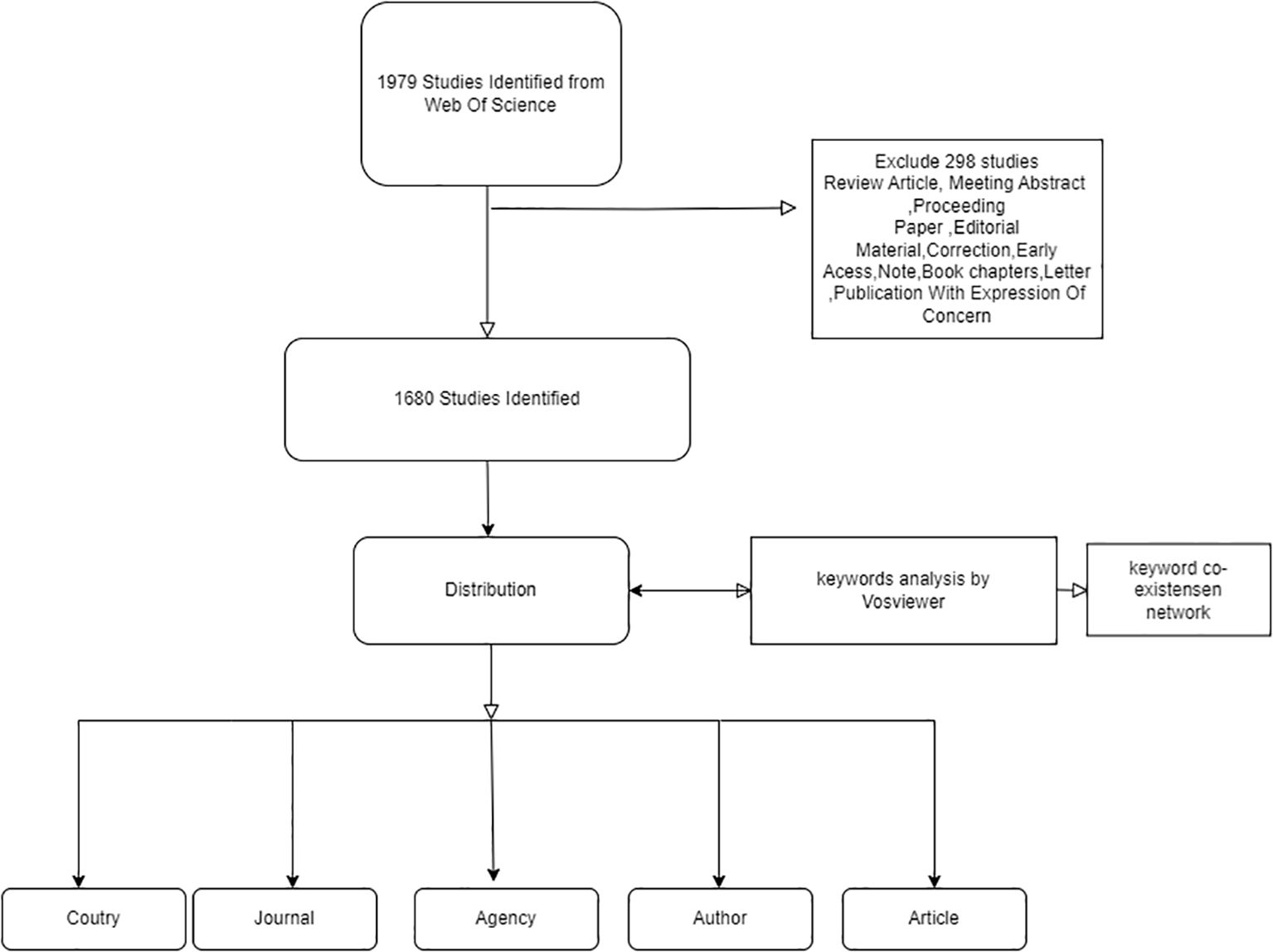
Figure 1. Inclusion and exclusion criteria for diabetes in osteocalcin studies.
Data collection and statisticsThe raw data downloaded from WoSCC was initially imported into Microsoft Excel 2019 for preliminary collation. Subsequently, two researchers (FZG and WJ) conducted independent verification assessments. In the event of discrepancies, the assessment was reassessed by a third party and immediately triangulated. Finally, the bibliometric parameters were extracted, namely the number of papers and citation frequency.
The statistical methods employed included importing the collated data into the bibliometric online analysis platform (https://bibliometric.com/) for statistical analysis of the total number.
A cluster analysis of keywords was conducted using VoS viewer, based on their occurrence in titles and abstracts (19). Furthermore, the frequency and interconnections of different keywords were described by the colour, size and connecting lines of the circles (20).
ResultAnnual scientific productionAs illustrated in Figure 2- Line graph of the number of articles published over time., the earliest pertinent article was published in 1986. Between 1986 and 1990, the field is still in its infancy, with no more than five articles published each year. In 1991, there was a notable increase in the number of articles published, which can be attributed to the advancement of molecular biology techniques, such as the study of the osteocalcin gene sequence (21). This resulted in a scientific output that was greater than that of the previous five years combined. The period from 1991 to 2013 demonstrates a consistent upward trajectory, punctuated by fluctuations. The greatest increase in articles occurred in 2013, due to the proposal that “research was needed to define the role of osteocalcin and its carboxylated or under-carboxylated forms in the regulation of human glucose metabolism” (22). Consequently, as a consequence of the evolution of research themes, the annual scientific production of articles shows a decreasing trend, with two notable declines occurring in 2019 and 2023. In 2019, the majority of studies were related to osteoporosis, a complication of diabetes mellitus. The data from 2023 and 2024 are not relevant to the research topic due to the timing of the entry.
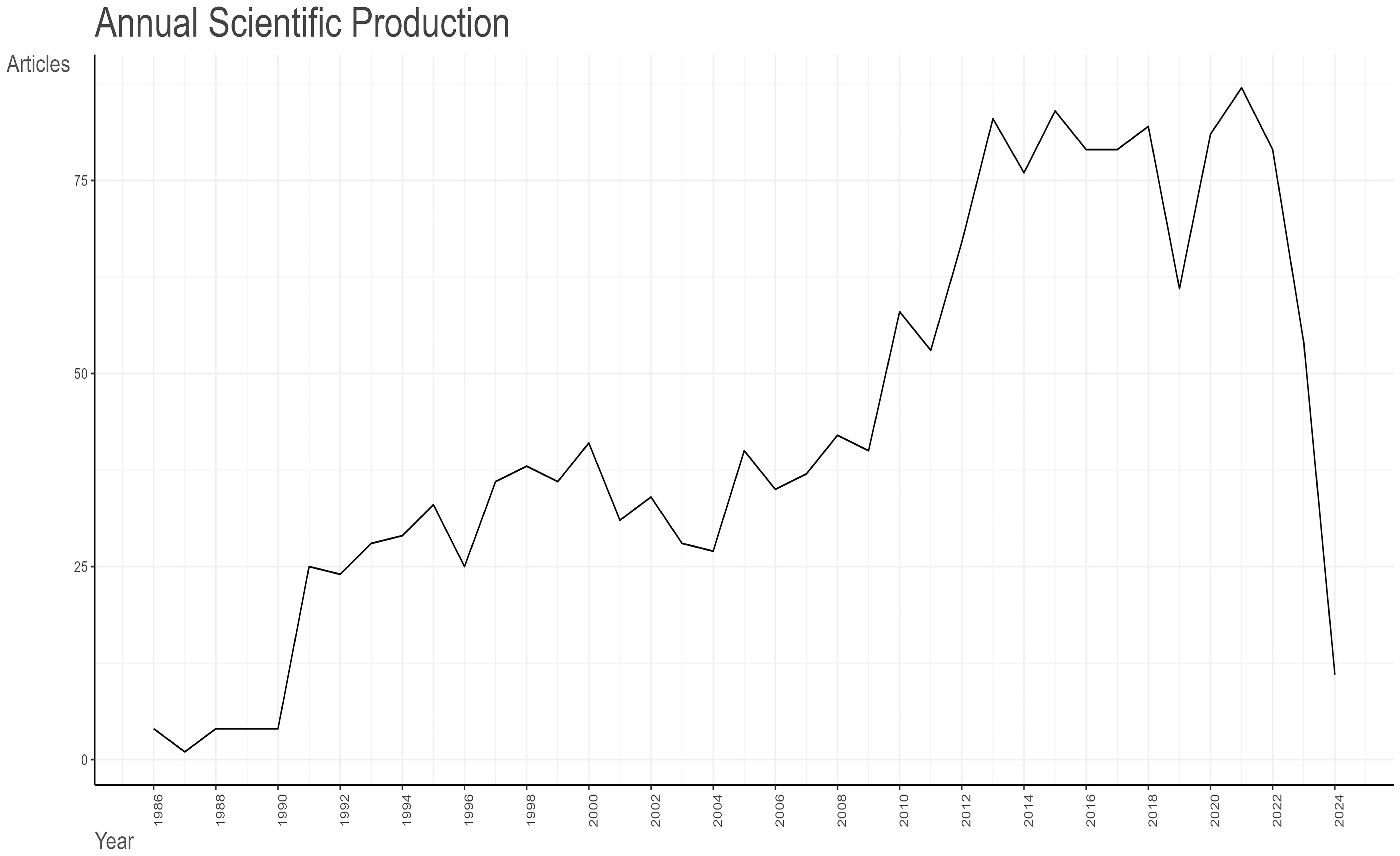
Figure 2. Line graph of the number of articles published over time.
Average number of citations per yearA total of 81,674 citations have been made of the 1,680 articles selected from the Web of Science (WoS) database, with an average citation frequency of 48.62 per article. As illustrated in Figure 3- A line graph showing the total citation volume per article over time., the peak of the average total citations per article was observed in 2007, with 120.76 citations per article as of 19 May 2024. This was followed by 2006, with 115.63 citations per article. Further analysis of the graph of the average number of citations per article per year in Table 1 Since 1986, the number of articles and citation counts in this field(MeanTCperArt means the mean number of total citations per article. N means the total number of articles in that year. MeanTCperYear means the mean number of MeanTCperArt per article) reveals that 2007 was the most prolific year, with an average of 6.71 citations per article per year. This was followed by 2006 (6.09), 2009 (5.24), and 2005 (5.21). 2010 ranked fifth, with an average of 4.83 citations per article per year and a total of 4,190 citations. In 2010, the literature was ranked fifth, with an average of 4.83 citations per article per year and a total of 4,199 citations, which placed it second only to the 4,468 citations in 2007. A detailed examination of these three types of data reveals the intricate nature of the influence of scholarly outputs and underscores the significance of a comprehensive assessment of the impact of the scholarly literature.
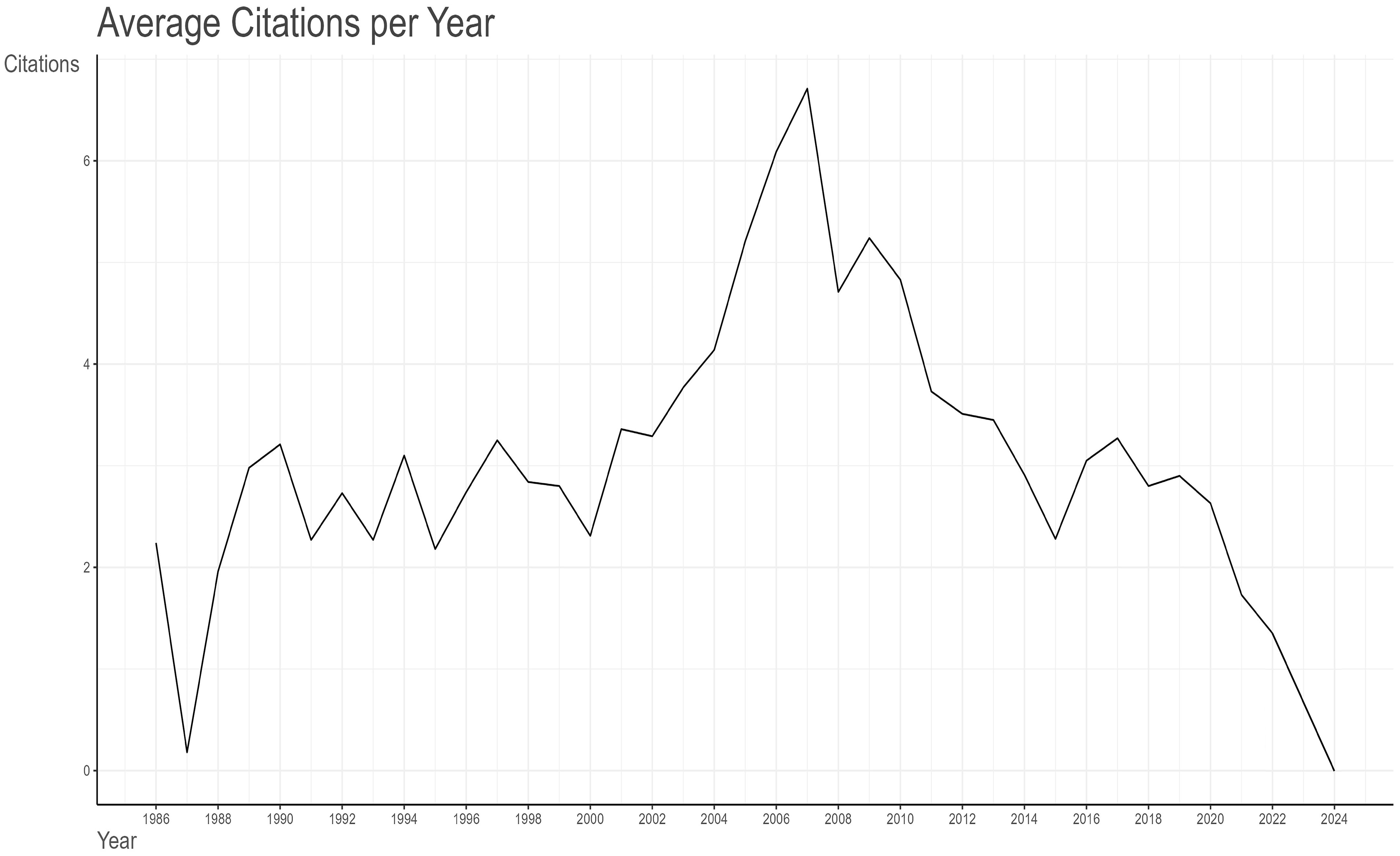
Figure 3. A line graph showing the total citation volume per article over time.
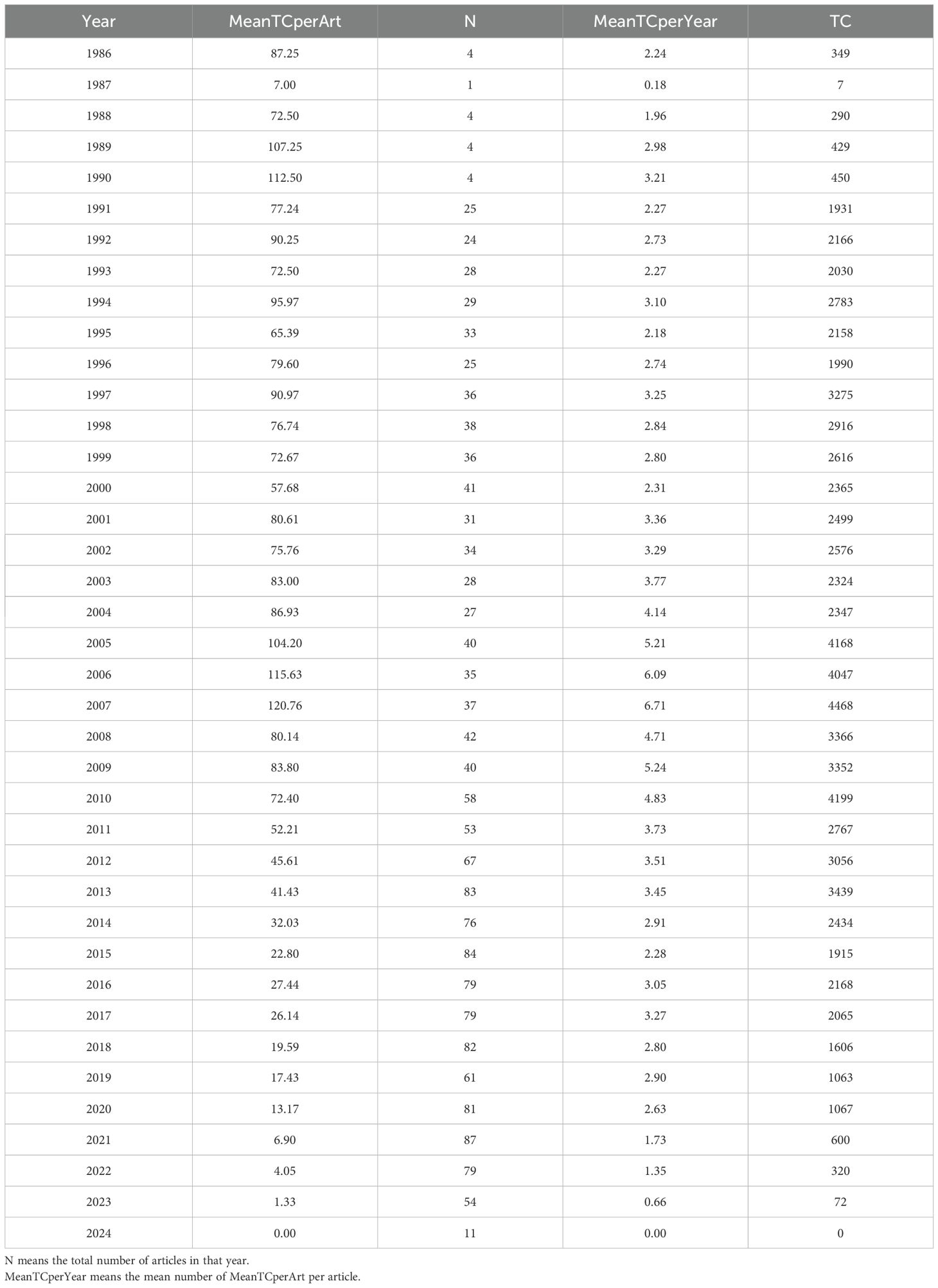
Table 1. Since 1986, the number of articles and citation counts in this field (MeanTCperArt means the mean number of total citations per article.
Quantity and citations among different nationsFigure 4 Analysis of research output in the field by various countries. The colour of the country represents the number of publications in that field. The darker the colour, the greater the number of articles published in that field. provides a global overview of the volume of scientific output in this field, with the United States accounting for the largest number of publications in this field. Table 2- Top 10 Countries with the Highest Productivity presents a comparative analysis of the performance of different countries in terms of scientific research output, based on three sets of data. The countries included in the analysis were selected based on their ranking in both the Countries’ Scientific Production and Most Cited Countries categories. The United States, with 2,411 scientific production articles, a total of 45,359 citations and an average citation rate of 81.7 citations, was at the top of the list, clearly outperforming China and Japan. China’s scientific production was 1,198 articles, with a cumulative total of 4,444 citations and an average citation rate of 16.5 citations. Japan’s scientific production amounted to 501 articles, with a cumulative total of 4,810 citations and an average citation rate of 37.6 citations, which is more than double that of China. The article with the highest number of citations in Japan was that which concluded that “osteocalcin was important not only for bone metabolism, but also for glucose and fat metabolism” (23). This was achieved by studying the parameters of atherosclerosis in men with type 2 diabetes mellitus and postmenopausal women. The highest number of citations for a single article in China was 198, and the article (24) concludes that “mucins could mimic the biological effects of insulin”.
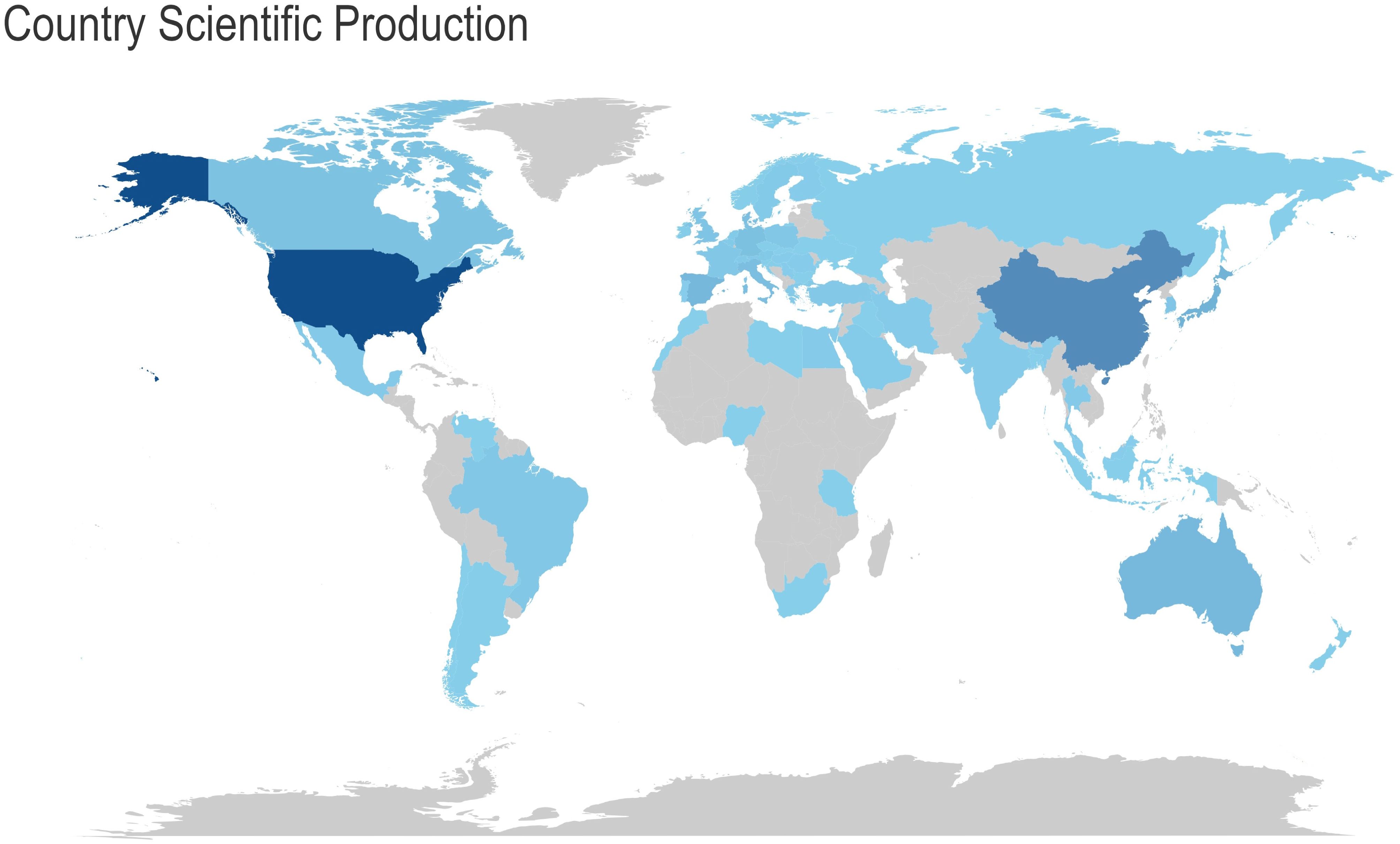
Figure 4. Analysis of research output in the field by various countries. The colour of the country represents the number of publications in that field. The darker the colour, the greater the number of articles published in that field.
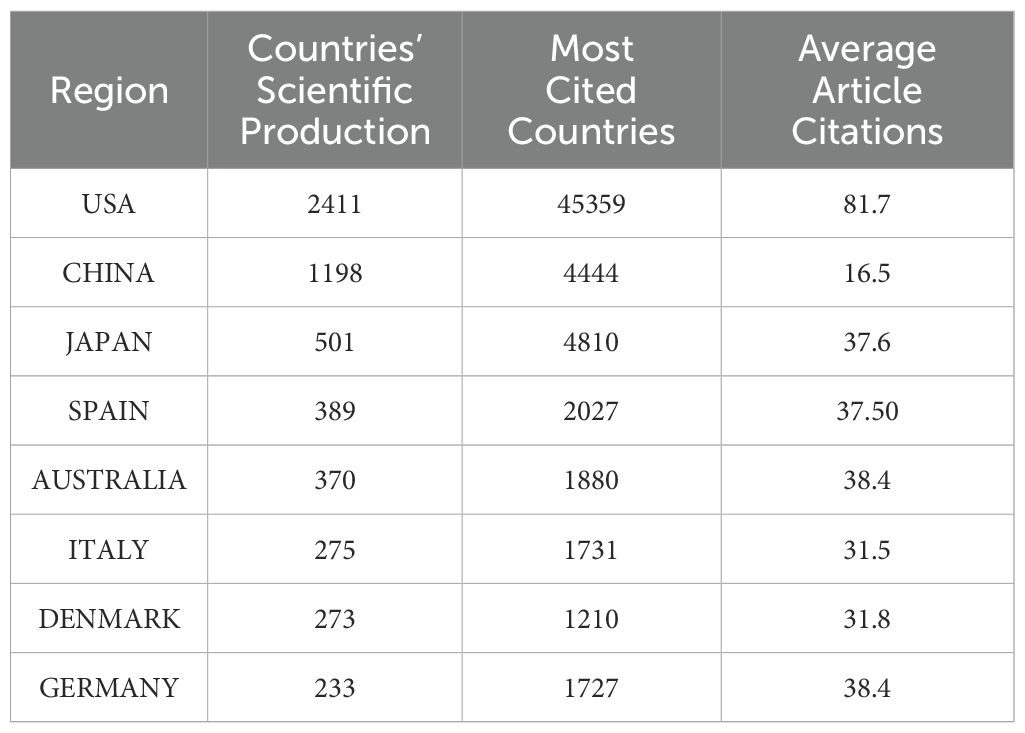
Table 2. Top 10 countries with the highest productivity.
As illustrated in Figure 5- Analysis of collaboration objectives among nations, with lines indicating cooperation projects between two countries, the United States had the greatest number of interrelated targets (36 countries, including China, Italy, Canada, the United Kingdom, Japan, Germany, France, and others) in terms of country cooperation. It is recommended that efforts be intensified to reinforce international cooperation and communication.
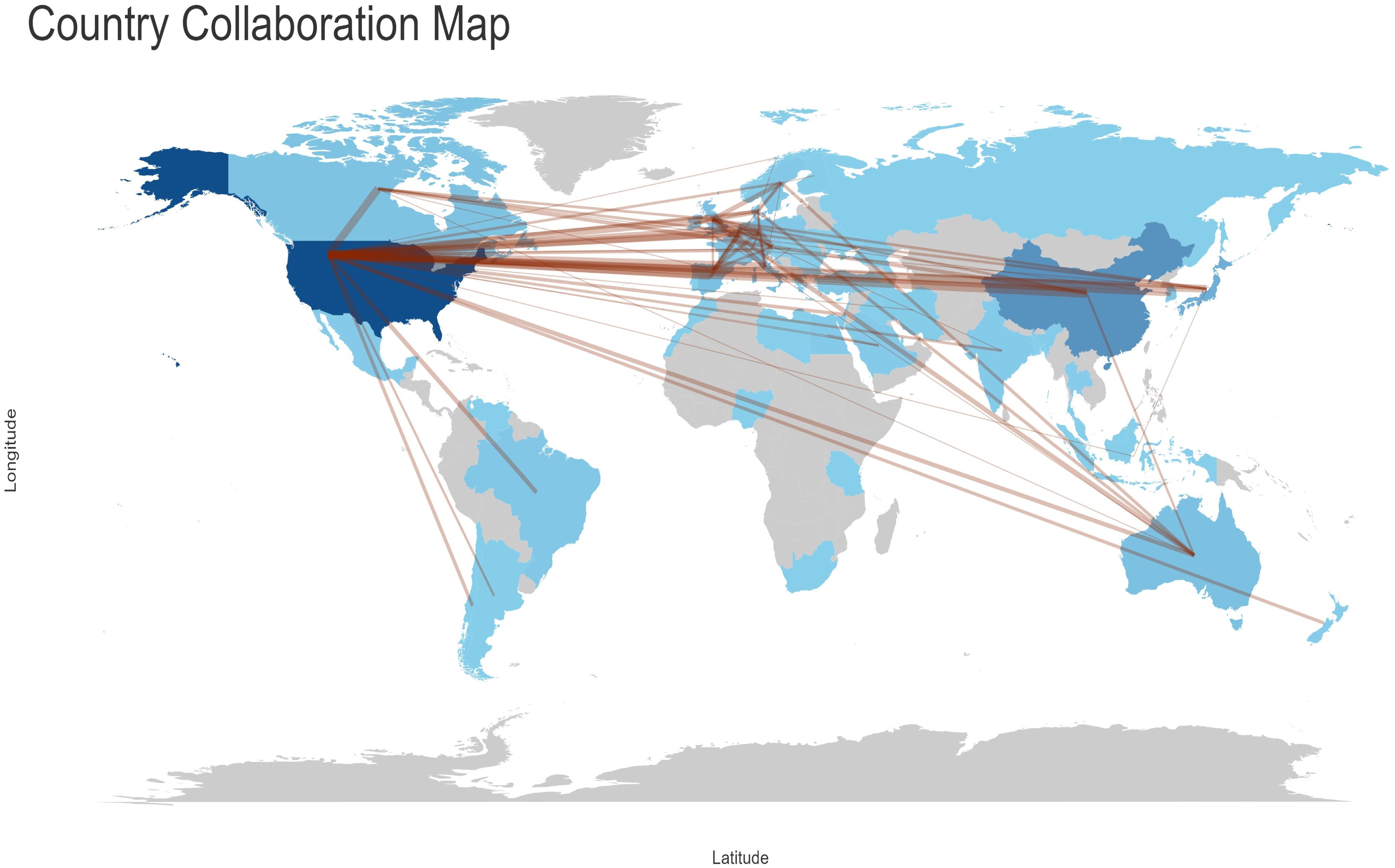
Figure 5. Analysis of collaboration objectives among nations, with lines indicating cooperation projects between two countries.
High contribution journalsThe top 10 journals by publication volume collectively published 576 articles, representing 34.29% of the total (Table 3- Top 10 Relevant Popular Journals). Among the journals, the Journal of Clinical Endocrinology & Metabolism had the highest number of publications (105 articles) and the most total articles published (89,559). Meanwhile, the Journal of Bone and Mineral Research had the highest Journal Citation Indicator (JCI) (1.38) and Impact Factor (6.2).
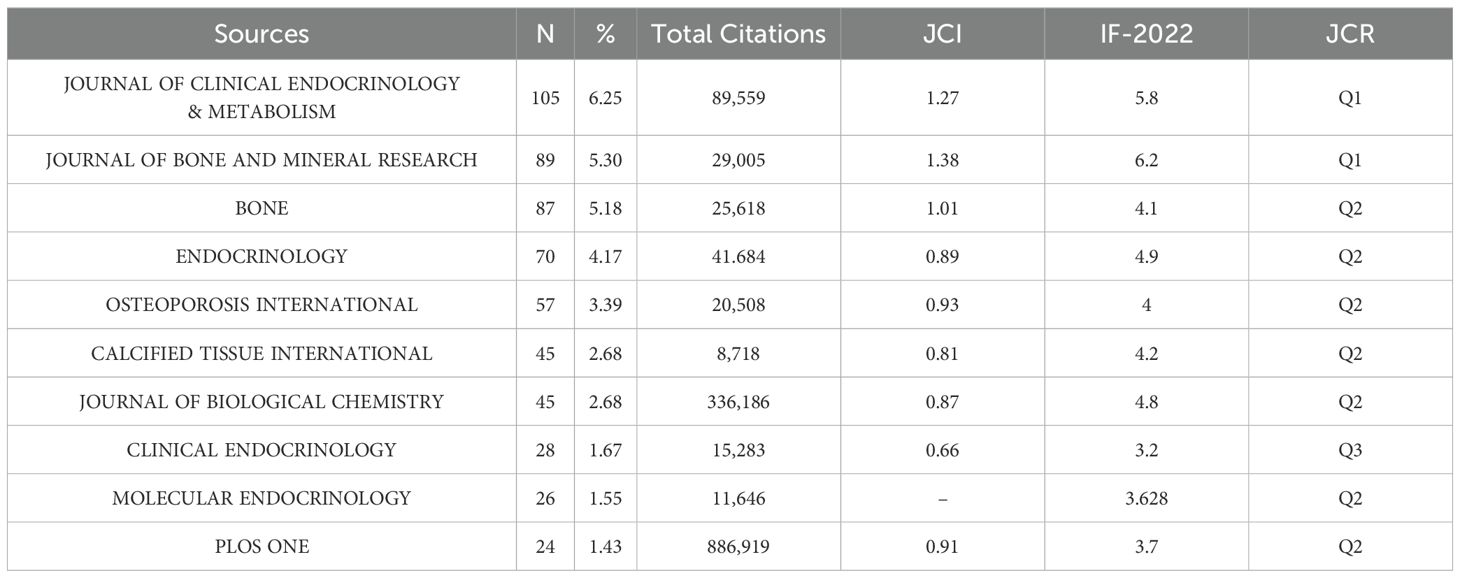
Table 3. Top 10 relevant popular journals.
The number of articles published by different institutionsIn terms of the number of publications, Harvard University in the United States is the leading institution, with 53 articles, as illustrated in Figure 6- Statistical analysis of the number of articles published by institutions. The larger the cluster, the more articles. Columbia University follows with 51 articles. The third-ranked institution is Shanghai Jiao Tong University from China, with 50 articles, which also represents the highest number of publications from a single institution in China. Among the top ten research institutions, eight are from the United States, with the remaining two being Shanghai Jiao Tong University from China and Shimane University from Japan.
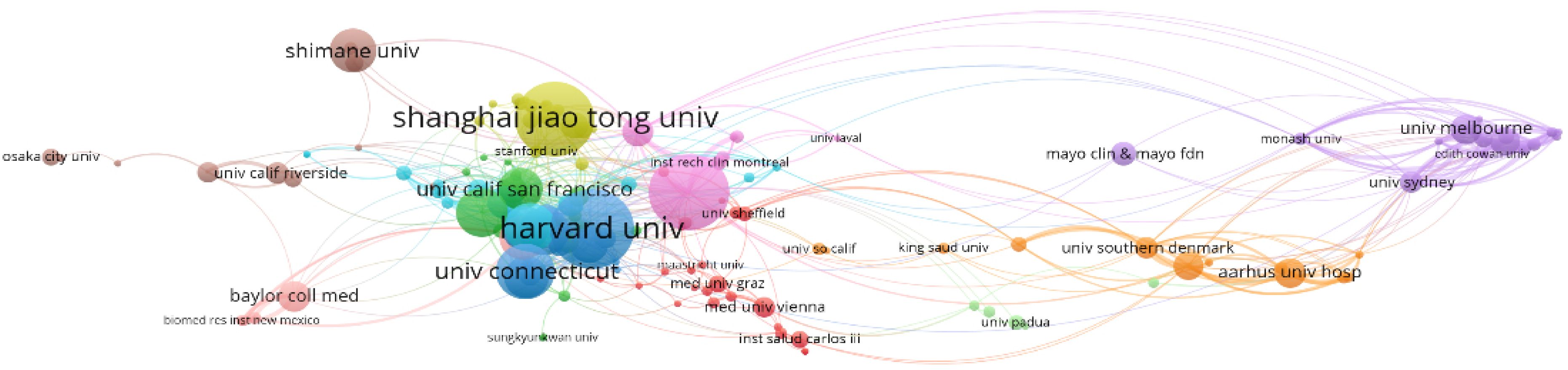
Figure 6. Statistical analysis of the number of articles published by institutions. The larger the cluster, the more articles published.
Collaboration networkThe author collaboration network graph generated by Bibliometrix has eight clusters after excluding individual authors as clusters. The first cluster is purple, the second is blue, the third is pink and the fourth is grey. The first group consisted mainly of Chinese researchers from Shanghai Jiao Tong University (SJTU), and its core Figure was Prof. Yuxian Bao, who had the strongest collaborative relationship among the four of them, namely Academician Weiping Jia, Prof. Xiaojing Ma and Scholar Yiting Xu. It should be noted that the graph shows that the scholar in the first group, Jing Zhang, had made contact with the second group, but subsequent checking of the information revealed that the researcher working with Prof Bao in the first group was from SJTU, and the researcher working with L R McCabe in the second group was from Michigan State University. The names of these two people are repeated, resulting in an assignment error. Meanwhile, the first group shown in Figure 7-Collaborative relationships among authors. Divided into 8 clusters, the connections between nodes indicate the existence of collaboration, with the thickness of the lines representing the strength or frequency of the collaboration. The author names at the centre of each cluster represent the key Figures of that cluster. worked closely with the fourth group. However, due to the abbreviation of the names, Xinmei Zhang collaborated with Prof. Levinger, Itamar in group 4, and Xiaohui Zhang collaborated with Prof. liu y, neither of whom was from SJTU. The liu y in the fourth group also refers to different people, which does not indicate that the first and fourth groups worked closely together. The second group was led by Prof. Stein, Gary S. from the University of Vermont, and had close cooperation with Prof. Lian, Jane B. and Prof. Stein, Janet L. The members of this group came from different research institutions in the United States, such as the University of Vermont, the University of Massachusetts, Harvard University, the University of Wisconsin, and Michigan State University, and so on. In Figure 7-Collaborative relationships among authors. Divided into 8 clusters, the connections between nodes indicate the existence of collaboration, with the thickness of the lines representing the strength or frequency of the collaboration. The author names at the centre of each cluster represent the key Figures of that cluster., the members of the second group worked closely with the third group. In fact, it is Prof. Yamauchi, Miki, who had collaborated with the members of the second group, not Yamauchi, Mika, who was the researcher of the third group, and the central Figure of the third group was Prof. Sugimoto, Toshitsugu of Shimane University, who had collaborated with Prof. Kanazawa, Ippei, Prof. Yamauchi, Mika, and Prof. Yamaguchi, Mika. Professor Sugimoto, Toshitsugu of Shimane University, who had a strong collaborative relationship with Professor Kanazawa, Ippei, Professor Yamauchi, Mika and Professor Yamaguchi, Toru, and the four of them had a total of seven articles related to the topic of this paper on the Web of Science, compared with the four in the first group who had a total of eight articles related to the topic of this paper.
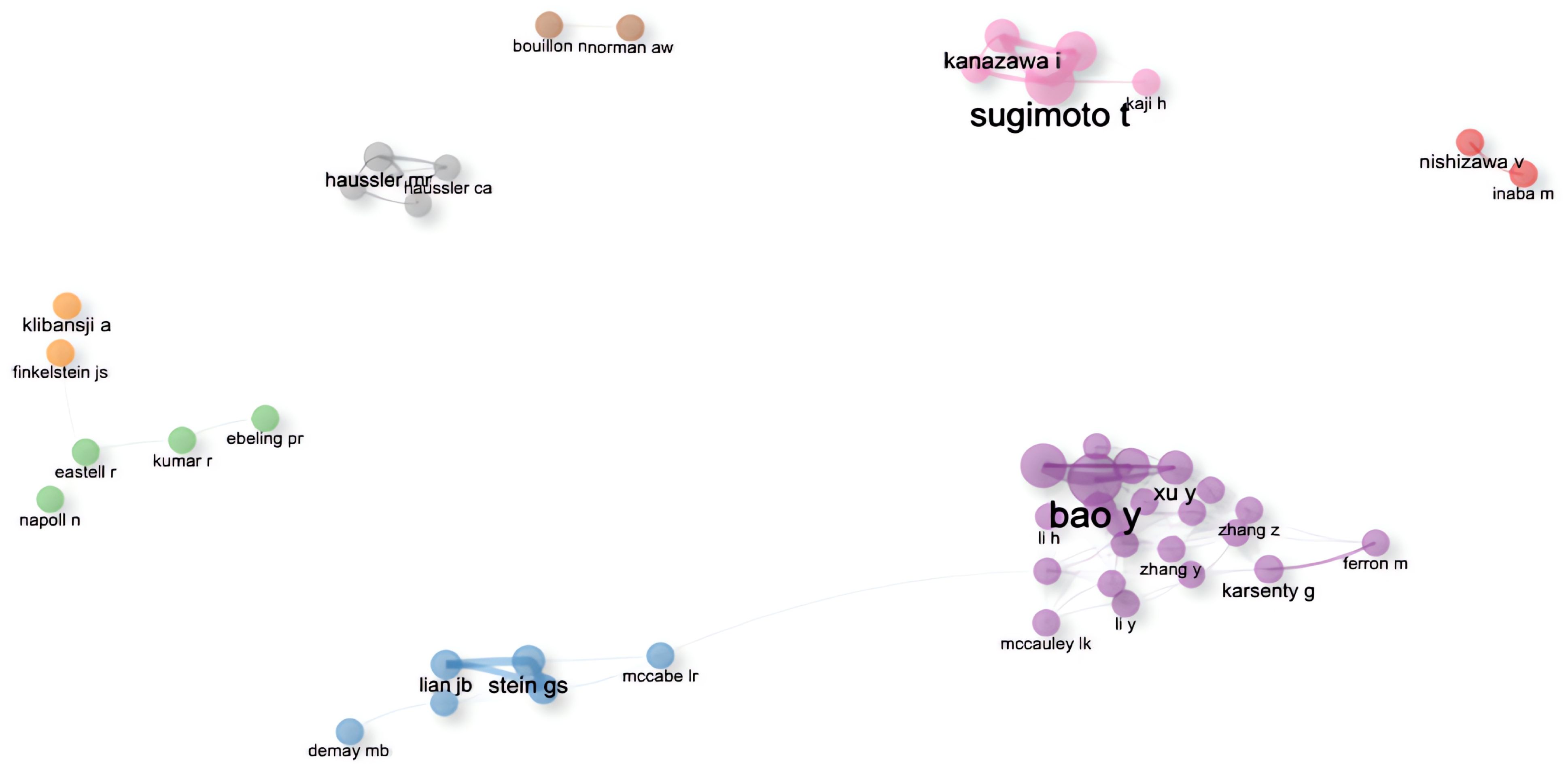
Figure 7. Collaborative relationships among authors. Divided into 8 clusters, the connections between nodes indicate the existence of collaboration, with the thickness of the lines representing the strength or frequency of the collaboration. The author names at the centre of each cluster represent the key Figures of that cluster.
Keywords have been filtered from the existing data, resulting in 395 words, which can be divided into four clusters, as it is shown in the Figure 8-Keywords scientific analysis Cluster 1, “Expression and Function of the Osteocalcin Gene,” is represented by green. Cluster 2, “Differential Expression of the Osteocalcin Gene and Its Impact on Diabetes,” is represented by blue. Cluster 3, “Role of Osteocalcin in Bone Turnover,” is represented by red. Cluster 4, “Indirect Involvement of Osteocalcin in Metabolic Processes,” is represented by yellow. The size of the keyword circles within each cluster corresponds to their frequency of occurrence.
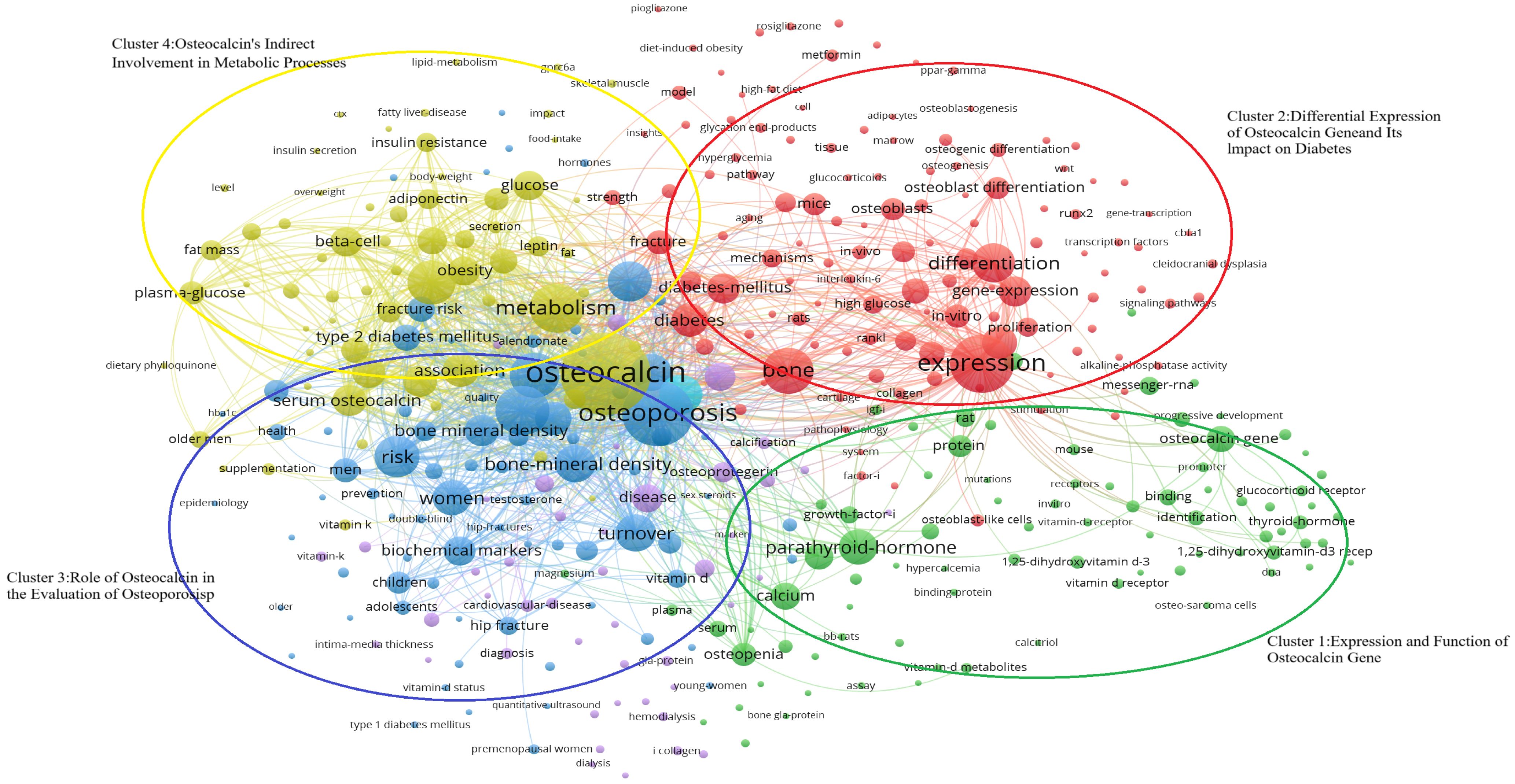
Figure 8. Keywords scientific analysis clustering. (Cluster 1:Expression and Function of Osteocalcin Gene; Cluster 2:Differential Expression of Osteocalcin gene and Its Impact on Diabetes; Cluster 3;Role of Osteocalcin in the Evaluation of Osteoporosis; Cluster 4:Expression and function of Osteocalcin’s Indirect Involvement in Metabolic Processes).
The main terms constituting cluster 1 are “osteocalcin gene” (25, 26), “protein” (27, 28), “parathyroid hormone” (29, 30) and “1,25-dihydroxyvitamin-D3 receptor” (29, 31). Meanwhile, cluster 2 is primarily characterized by “expression” (25, 26), “difference” (25, 32), “diabetes” (33, 34) and “osteoblast” (31, 35). Cluster 3 focuses on keywords such as “osteoporosis” (36, 37), “bone turnover” (38, 39), “male” (40, 41), and “female” (42, 43). Lastly, cluster 4 includes keywords like “osteocalcin” (37, 44), “metabolic syndrome” (45, 46), “insulin resistance” (33, 47), and “plasma glucose” (41, 44).
VoS viewer marks keywords in the graph with different colours based on the average year of occurrence, with purple keywords appearing earlier than blue and yellow ones. The transition from purple to green and finally to yellow illustrates the developmental process of the keywords. The graph provides a comprehensive overview of the researchers’ investigation focus, including four clusters of keywords such as “Expression and Function of Osteocalcin Gene,” “Differential Expression of Osteocalcin Gene and Its Impact on Diabetes,” “ Role of Osteocalcin in the Evaluation of Osteoporosis and Diabetes” and “Osteocalcin’s Indirect Involvement in Metabolic Processes.”
Through bibliometrics, one can quantitatively and systematically assess trends in a specific field and predict potential research directions, as it is shown in the Figure 9-. In this study, keywords were categorized into four clusters:
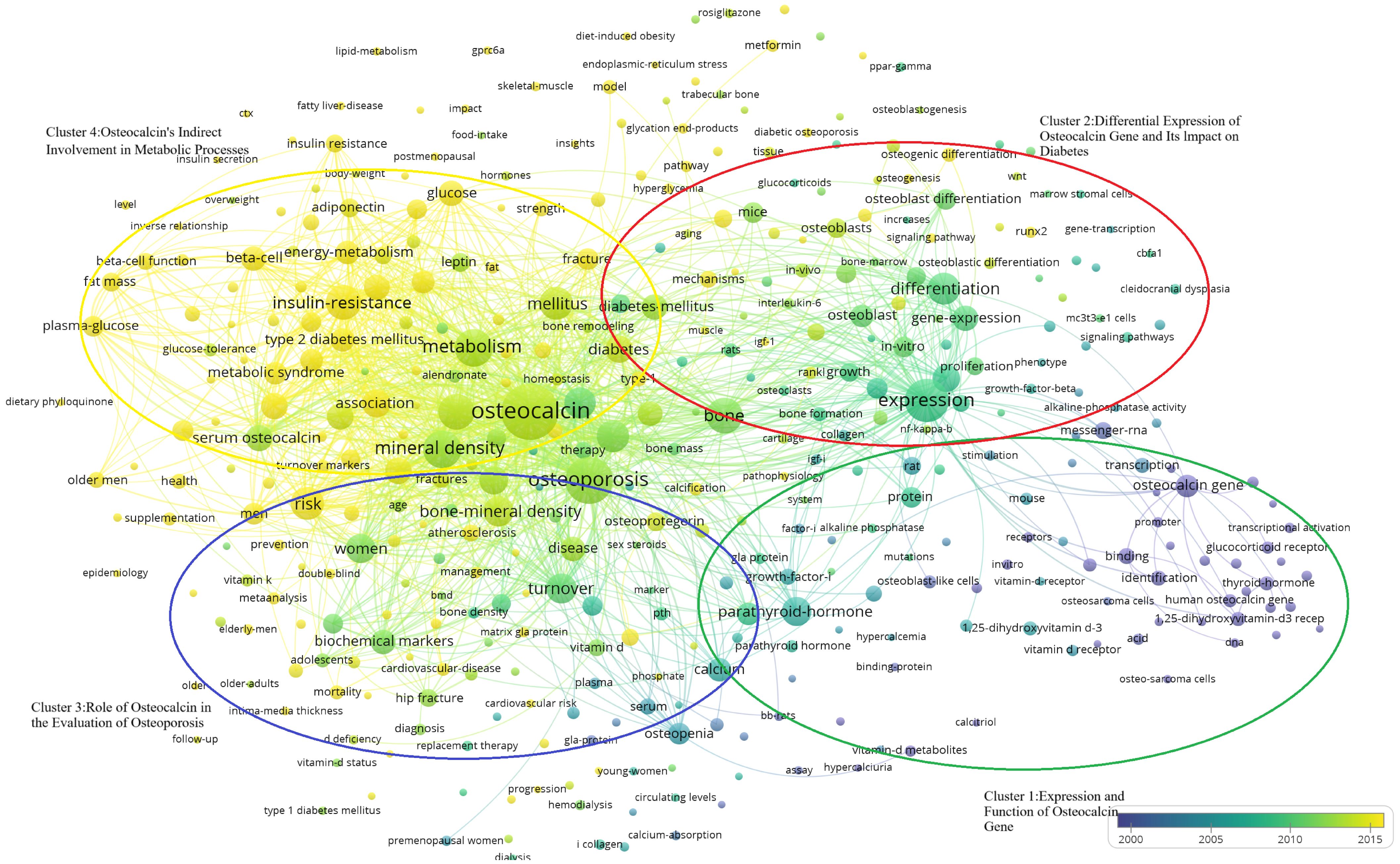
Figure 9. Temporal distribution of the four keyword clusters. (Cluster 1:Expression and Function of Osteocalcin Gene; Cluster 2:Differential Expression of Osteocalcin gene and Its Impact on Diabetes; Cluster 3;Role of Osteocalcin in the Evaluation of Osteoporosis; Cluster 4:Expression and function of Osteocalcin’s Indirect Involvement in Metabolic Processes).
“Expression and Function of Osteocalcin Gene”(Cluster 1, Green) “Differential Expression of Osteocalcin Gene and Its Impact on Diabetes”(Cluster 2, Blue) “ Role of Osteocalcin in the Evaluation of Osteoporosis and Diabetes”(Cluster 3, Red) “Osteocalcin’s Indirect Involvement in Metabolic Processes”(Cluster 4, Yellow). In the Figure 9-, it shows that the researchers’ investigative interests shifted from Cluster 1 to Cluster 2, then to Cluster 3, and finally to Cluster 4.
Characteristics of the top 10 most cited research articlesThe 10 most cited articles were cited a total of 8493 times (10.40%, Temporal distribution of the four keyword clusters. (Cluster 1:Expression and Function of Osteocalcin Gene; Cluster 2:Differential Expression of Osteocalcin gene and Its Impact on Diabetes; Cluster 3;Role of Osteocalcin in the Evaluation of Osteoporosis; Cluster 4:Expression and function of Osteocalcin’s Indirect Involvement in Metabolic Processes) (Figure 10- Top 10). The third most cited article was a review, and Prof. Na Kyung Lee’s 2007 article (48) ranked first in both total citations and citation frequency per year, with 1902 and 105.67, respectively. This article accounted for 42.6% of the total citations in 2007. In 2005, articles by Tripti Gaur (26) and Christina N Bennett (28) ranked second and seventh in total citations, with 923 and 702, respectively. These two articles combined account for 38.99% of the citations for the year. Mathieu Ferron’s articles in 2010 (27) and 2008 (25) ranked fourth and sixth at 831 and 721, respectively, accounting for 19.79% and 21.42% of that year’s articles. His two articles accounted for 18.27% of the 10 most cited articles. Thus, the average number of citations per year is determined by a combination of annual scientific output and high-impact articles, with the latter playing a more pronounced role. The ten articles are presented in Table 4-Top 10 Most Cited Research Paper for the reader’s convenience.
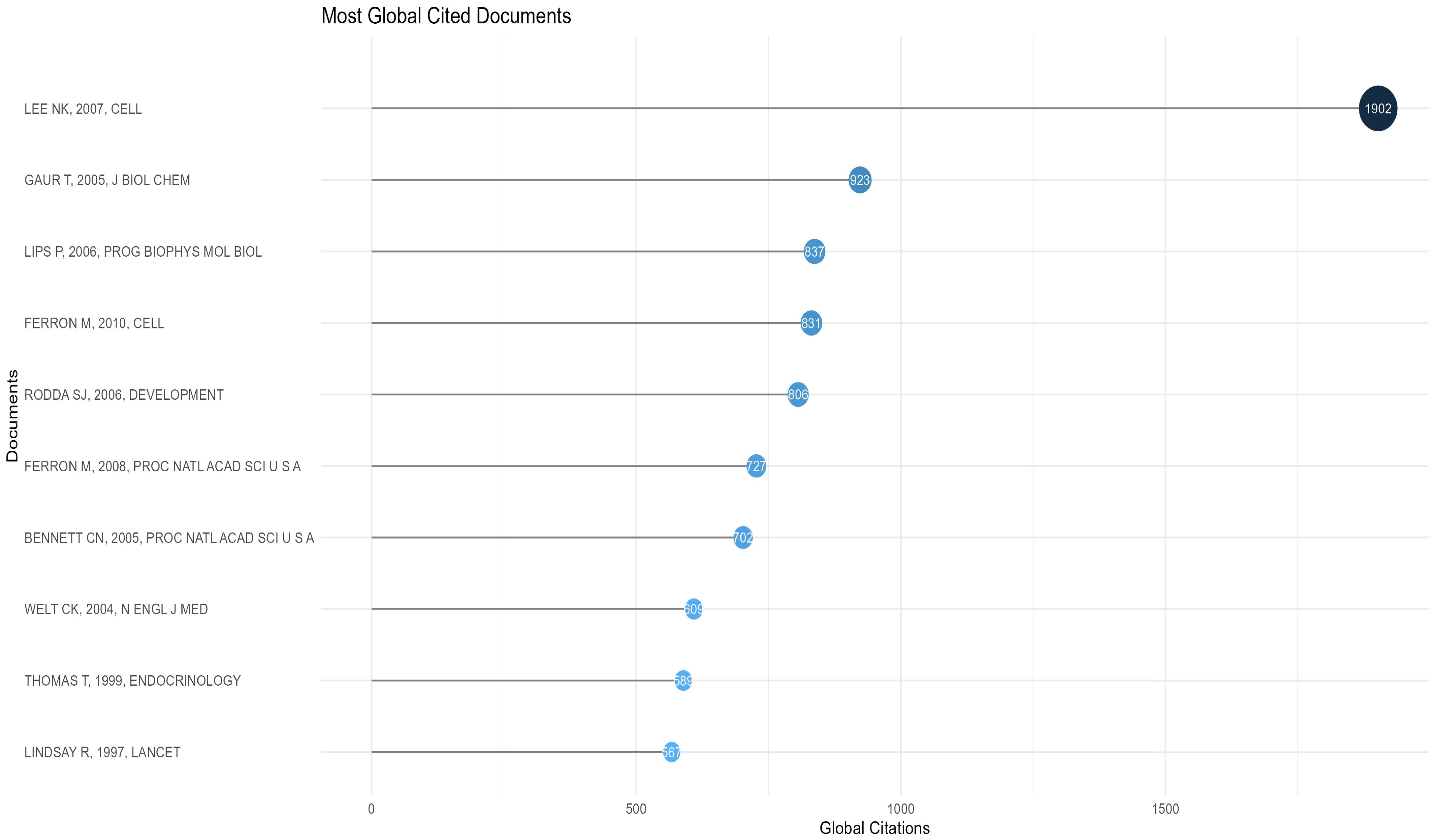
Figure 10. Top 10 most global cited articles.
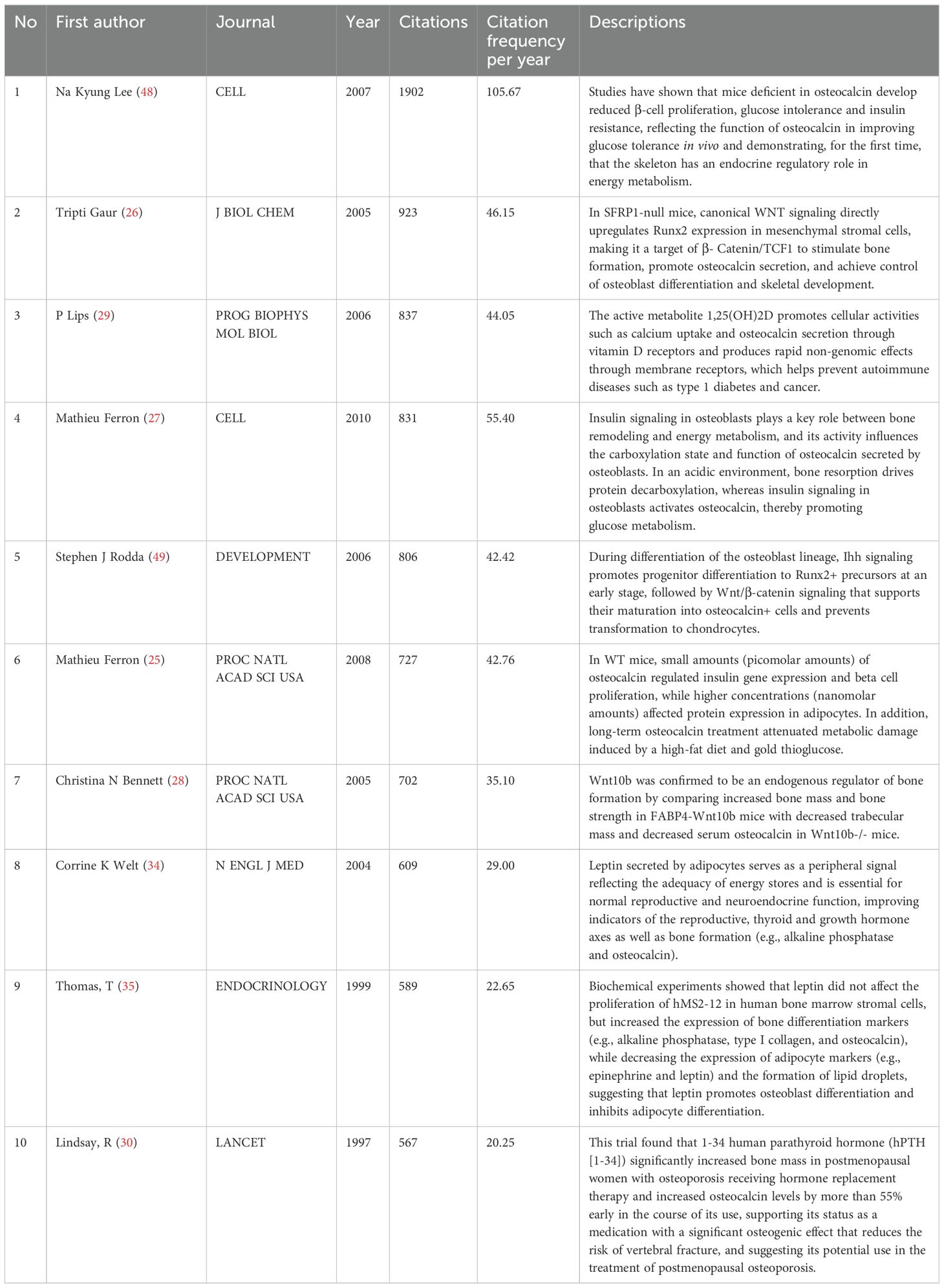
Table 4. Top 10 most cited research paper.
DiscussionExpression and function of osteocalcin geneAs shown in Figure 8-Keywords scientific analysis In cluster 1, the main terms are “osteocalcin gene”, “protein”, “parathyroid hormone”, “thyroid hormones” and “1,25-dihydroxy vitamin-D3 receptor”. This group of terms is summarized as the physiological mechanism where osteocalcin interacts with other hormones.
Osteocalcin exerts an influence on the absorption and regulation of calcium, operating in conjunction with other hormones. It has been demonstrated that thyroid hormone (TSH) exerts a pivotal influence on bone growth and development (50). The thyroid glands secrete substantial quantities of thyroxine (T4) and 3,5,3′-triiodothyronine (T3). Although the circulating levels of T3 are considerably lower than those of T4, T3 activates T3 receptors (TRα and TRβ) on osteoblasts, thereby stimulating osteocalcin secretion (51). Further investigation has revealed that TRα is the predominant isoform expressed in bone tissue, while TRβ deficiency results in a hyperthyroid effect in osteoblasts (52). Although T4 does not have as strong an affinity for the receptor as T3 (53), it has also been demonstrated in experimental studies that its osteoblastic differentiation can have a stimulatory effect (51). Furthermore, T4 and T3 have been demonstrated to directly stimulate bone resorption in vitro (54). Furthermore, one study indicates that estrogen status may influence the TSH response to bone (55), which could potentially elucidate the elevated prevalence of osteoporosis observed in postmenopausal women. As a consequence of TSH suppression and elevated FT4 and/or free triiodothyronine (FT3) levels in hyperthyroid patients, there is an increased rate of bone conversion, a reduction in bone mineral density (BMD), and an elevated risk of fragility fractures (56). A controlled trial of a cohort of patients with hyperthyroidism, hypothyroidism, and euthyroidism revealed that blood osteocalcin levels were markedly elevated in the hyperthyroid group and markedly reduced in the hypothyroid group when compared to the euthyroid control group (57). In patients with hyperthyroidism, antithyroid hormone medication has been demonstrated to reduce blood osteocalcin concentrations. Conversely, in patients with hypothyroidism, L-T4 has been shown to be an effective means of restoring osteocalcin levels (58). It has been demonstrated that thyroid hormone can facilitate osteocalcin synthesis in osteoblasts by activating p38 MAP kinase (59). Consequently, the thyroid hormone plays a pivotal role in regulating bone function, and influencing bone metabolism. Hyperthyroidism is a recognized cause of secondary osteoporosis (60), which is characterized by accelerated bone turnover and a negative calcium and phosphorus balance (61). In addition to its role in bone conversion and formation, the promotion of osteocalcin synthesis, which leads to increased bone conversion, may also be a pathway by which hyperthyroidism causes osteoporosis.
With regard to parathyroid hormone (PTH), it is once more an essential peptide hormone that regulates bone formation and osteoblast activity. Parathyroid hormone is capable of regulating extracellular calcium and phosphorus levels and stimulating bone resorption. Two principal pathways are responsible for the regulatory effects of parathyroid hormone on bone: the PKA pathway and the PKC pathway. The regulatory effects of parathyroid hormone on bone are mediated by direct activation of parathyroid hormone receptor 1 (PTHR1) on osteoblasts, which stimulates Gαs-mediated activation of adenylate cyclase and promotes the production of cAMP, followed by the activation of protein kinase (PKA) (62). Subsequently, the activation of the Raf-MEK-ERK mitogen-activated protein kinase (MAPK) cascade reaction (63) results in a proliferative effect on bone (64). Furthermore, the production of cAMP and the activation of PKA can also activate Gq/11-mediated PLCβ stimulation, which in turn leads to the production of inositol 1,4,5-trisphosphate (IP3), the mobilization of calcium and the activation of protein kinase C (PKC) (65). PKC then activates MAP kinase and exogenous signal-regulated kinase (ERK), which in turn results in the onset of osteoblast proliferation (64). Furthermore, it has been demonstrated that parathyroid hormone can act synergistically through the PKA and PKC pathways to co-stimulate osteocalcin gene expression in osteoblasts (66). This pathway directly activates osteoblast OCN gene transcription by facilitating the binding of the OSE1 sequence proximal to the mOG2 promoter to nuclear proteins (67). Clinical trials have demonstrated that increased parathyroid hormone levels lead to elevated osteocalcin levels (68) and are effective in ameliorating idiopathic osteoporosis in men (69). Notably, several experiments have shown that both instantaneous and intermittent administration of parathyroid hormone are effective in stimulating bone formation and repair (70, 71), which appears to be related to the gradient sensitivity of parathyroid hormone (71).
OSE2 is a specific cis-acting element present in osteoblasts, and Osf2/Cbfa1 is a protein that binds to OSE2, regulated by Bone Morphogenetic Protein 7(BMP7) and Vitamin D-3. Osf2/Cbfa1 binds to and regulates the expression of multiple genes in osteoblasts (72). Research indicates that 1,25D regulates bone mineral remodelling by inducing Receptor Activator of Nuclear Factor κB Ligand(RANKL), Secreted Phosphoprotein 1 Gene(SPP1), and Bone Gla Protein(BGP), and also controls calcium and phosphorus reabsorption in the kidneys, with the skeleton acting as a sensor for phosphorus levels (73). Upon binding with the Vitamin D receptor, 1,25-dihydroxyvitamin D3(1,25D) directly inhibits parathyroid hormone gene transcription and antagonizes osteocalcin to prevent hypercalcemia (29). Controlling osteocalcin expression may delay age-related chronic diseases such as osteoporosis, type 2 diabetes, cardiovascular disease, and cancer.
While not directly involved in bone mineralization, osteocalcin has been identified as a factor that plays a role in preventing excessive bone mineralization and increased bone fragility in osteoporosis. The absence of osteocalcin in experimental animals led to the observation that, despite the normal survival of osteocalcin-free mutant mice, their cortical bone width was significantly higher than that of the wild type after six months. This was observed in the absence of an increase in osteoclast number, mineralization rate, and bone mineral content (74). This indicates that osteocalcin is not a factor in the process of mineralization. Subsequently, the researchers induced osteoporosis in the mutant and wild-type mice by removing their ovaries. This resulted in more pronounced osteoporosis symptoms in the mutant mice than in the wild-type, which may be attributed to an increased number of osteoclasts in the mutant mice. This indicates that osteocalcin exerts its effect by limiting bone matrix formation, without influencing resorption or mineralization. The relative amount of hydroxyapatite phosphate is diminished in osteocalcin-deficient mice, which exhibit reduced bone maturation (75), indicating that osteocalcin deficiency may be associated with increased bone fragility. It may therefore be posited that the administration of vitamin K (76), 1,25-dihydroxy-D3 (77) to patients exhibiting low osteocalcin levels may prove an efficacious method of reducing the risk of osteoporosis, particularly in those already diagnosed with the condition. In the context of long-term warfarin anticoagulation, the potential for reducing the risk of osteoporosis may be realized through the replacement of warfarin with a non-vitamin K-dependent anticoagulant, such as dabigatran (78).
The association between osteocalcin levels and type 2 diabetes has been demonstrated in numerous studies across diverse populations (36, 79, 80). In animal experiments, it has been demonstrated that osteocalcin is associated with the regulation of blood glucose levels and improved insulin sensitivity and secretion (48). Intermittent osteocalcin injections have been shown to increase glucose tolerance and insulin sensitivity, improve pancreatic β-cell mass, and prevent hepatic steatosis in mice (44). While this treatment regimen has not yet been implemented in clinical practice (81), it represents a promising avenue for future diabetes treatment and prevention strategies.
Despite evidence from statistical experiments indicating a potential correlation between osteocalcin and cardiovascular disease (82–85), the precise mechanism of action remains unclear. Osteocalcin has been shown to exert protective effects on the vascular endothelium in both animal (86) and in vitro (87) experiments. The transformation of vascular smooth muscle cells into osteoblast-like cells is a key mechanism underlying vascular calcification in advanced atherosclerosis (88). Higher osteocalcin levels were observed in calcified plaques and aortic valves (89), and there was a positive correlation between vascular smooth muscle cell shift to osteoblast-like cells and osteocalcin expression (90). However, a clinical meta-analysis has indicated that in certain cardiovascular diseases, particularly atherosclerosis, no discernible correlation was observed between osteocalcin and markers of atherosclerosis and calcification (91). In contrast, studies of young adults have revealed a strong correlation between osteocalcin and cardiovascular disease, with this association becoming more pronounced with age (92). Given the role of osteocalcin in improving blood glucose, blood lipids and alleviating diabetes, its effects may be indirect and related to the regulation of blood glucose and lipid levels and metabolism. Despite the fact that numerous experiments have demonstrated that the role of osteocalcin in cardiovascular diseases is complex and still unclear, further research is required, the close association between osteocalcin and some diseases, in particular atherosclerosis, may prove to be a significant breakthrough in this field.
Given the regulatory role of osteocalcin in bone formation and remodeling, there has been considerable interest in its association with tumors, especially primary bone tumors. A reduction in osteocalcin expression has been observed in tumor cells in numerous animal experiments on osteosarcoma (93, 94). This may be associated with defective collagen fiber mineralization in osteosarcoma (95). Furthermore, rearrangements and loss of expression of the p53 gene have been observed in the vast majority of osteosarcomas (96). It has been postulated in animal studies that p53 rearrangement may contribute to the maintenance of a tumourigenic phenotype in osteosarcoma (93). Furthermore, it has been suggested that the p53 gene is a positive regulator of osteocalcin (97). It is therefore challenging to ascertain whether reduced osteocalcin levels contribute to elevated osteosarcoma incidence, whether increased osteosarcoma incidence is attributable to p53 rearrangements, or if both factors are involved. Further study is required to elucidate the precise effects of osteocalcin on osteosarcoma. While the precise role of osteocalcin in osteoblast differentiation remains unclear, its potential as a discriminating criterion for the degree of differentiation has been clinically validated (98). It is noteworthy that a viral toxicity therapy based on the intravenous injection of the osteocalcin promoter was observed to significantly inhibit the growth of osteosarcoma lung metastases and significantly improve survival in animal experiments (99). This appears to indicate that osteocalcin may also exert an inhibitory effect on osteosarcoma metastases. This offers a novel perspective on the potential treatment of osteosarcoma and its metastases.
Differential expression of osteocalcin gene in relation to diabetes mellitusCluster 2 is characterised by the core terms ‘expression’, ‘differential’, ‘diabetes’ and ‘osteoblasts’. In this group, differential gene protein expression in osteoblasts may be associated with diabetes and the development of diabetic bone disease.
On the one hand, bone trap cells, osteoblasts produce rankl which is an important factor for osteoclast differentiation and activation (100), and osteoclasts have an extremely important role for the conversion of osteocalcin to ucOC, and ucOC has an effect on insulin that enhances its sensitivity phenotype, so that osteoblasts have an indirect regulatory role for insulin and glucose. In diabetic patients, high blood glucose decreases osteoblast and osteoclast activity, and Wittrant, Y. et al. showed that high blood glucose inhibits osteoclast formation, which may be due to the inhibition of redox-sensitive NF-kappaB activity through antioxidant mechanisms to alter RANKL-induced osteoclast formation (101).
Also, in osteoblasts, sympathetic tone stimulates the expression of Esp, a gene that inhibits osteocalcin activity by acting on its own to reduce osteocalcin secretion (102). In addition, the transcription factors forkhead box O1 (Foxo1) and activating transcription factor 4 (ATF4) inhibit osteocalcin metabolic activity by increasing ESP expression in osteoblasts (103). In a cross-sectional Danish study, Starup-Linde, J. et al. found that elevated non-fasting blood glucose levels were negatively correlated with p-CTX, p-P1NP, p-OC and p-ucOC, with the strongest effect being seen for hypo-carboxylated OC, which was reduced by 38% (104). In addition, the diabetes treatment drug, metformin, may ameliorate the inhibitory effect of hyperglycaemia on osteoblast proliferation and gene expression (105).
The role of inflammation in T2DM is unclear and may be indirectly mediated, whereby adipocytes can activate inflammation through the production of (ROS), which in turn increases the production of inflammatory cytokines that can reduce the number of osteoblasts and stimulate osteoclast bone resorption via apoptosis at the same time. Interestingly, this process becomes sustained as ROS stimulate MSCs to differentiate preferentially into adipocytes rather than osteoblasts, leading to a reduction in the transcription of Wnt proteins and further inhibiting bone formation (106).
The role of osteocalcin in the evaluation of osteoporosis and diabetesCluster 3 is characterized by the core terms “osteoporosis”, “bone turnover”, “male” and “female”. This group primarily elucidates studies on the association between bone alkaline phosphatase levels and 42 mixed gender patients(male and femal), including research on osteoporosis and diabetes.
Firstly, osteoporosis is an imbalance between the activities of osteoclasts and osteoblasts. Factors influencing this imbalance include calcium intake (25), vitamin D receptors (107), vitamin D receptors (107), physical activity or mechanical stress (108), hormones (parathyroid hormone, testosterone, estrogen) (109), and the Receptor Activator Of Nuclear Factor-Kappa-B Ligand(RANKL) (110).
Secondly, osteocalcin, as a Bone Turnover Marker(BTM), may serve as one of the criteria for evaluating the risk of osteoporosis. In cross-sectional studies of women, an increase in osteocalcin(OC) may reflect enhanced bone turnover, partially contributing to the development of osteoporosis (111). Moreover, in the diagnosis of osteoporosis, bone turnover markers(btms) can be widely used to improve prognosis and monitor the response to anti-resorptiv
留言 (0)