
記住我





The samples and data used for this analysis were obtained from a cohort of patients hospitalized at Geneva University Hospitals between January 2018 and July 2021. These patients were part of the OptimAT study. This single-center, prospective observational study (NCT03477331) was designed to optimize antithrombotic therapy in hospitalized patients using advanced pharmacokinetic modeling and was conducted in accordance with ICH Guidelines for Good Clinical Practice [10].
Additionally, data from healthy volunteers participating in the Geneva cocktail study (NCT01731067) were included as a control for Pgp activity [4]. The Geneva cocktail study aimed to evaluate the activity of six cytochrome P450 enzymes and Pgp using a specifically designed drug cocktail.
Both study protocols were approved by the regional research ethics committee of the Canton of Geneva (CCER ID: 2012–00085 and no. 2017-00225).
2.2 Study Design and Analytical MethodUpon inclusion, patients received capsules containing a low-dose cocktail following the validated Geneva cocktail procedure. The cocktail included bupropion (25 mg), flurbiprofen (25 mg), dextromethorphan (10 mg), omeprazole (5 mg), midazolam (1 mg), and fexofenadine (25 mg). Capillary whole blood samples (10 µL) were collected at baseline and 2, 3, and 6 hours post-administration. Blood was collected on Whatman 903 filter paper cards (Westborough, MA, USA) via finger prick using a BD Microtainer Contact-Activated Lancet (Plymouth, UK), with the volume measured using a volumetric micropipette (Rainin, Oakland, CA, USA). For this analysis, we focused exclusively on fexofenadine concentrations to investigate Pgp phenotypic activity.
Quantification of the cocktail substrates in dried blood spots was performed using a validated single reverse-phase high-performance liquid chromatography-tandem mass spectrometry method, operating in dual electrospray ionization mode, as previously described by Bosilkovska et al. [4].
2.3 Population Pharmacokinetic AnalysisThe popPK analysis was conducted using the stochastic approximation expectation maximization (SAEM) algorithm of the nonlinear mixed-effects modeling software MONOLIX (version 2021.1.0) [11]. A classical stepwise approach was adopted to identify the final model. Data management, statistical analysis, and graphical outputs were performed using R software (version 4.2.1; RStudio version 1.4.1717).
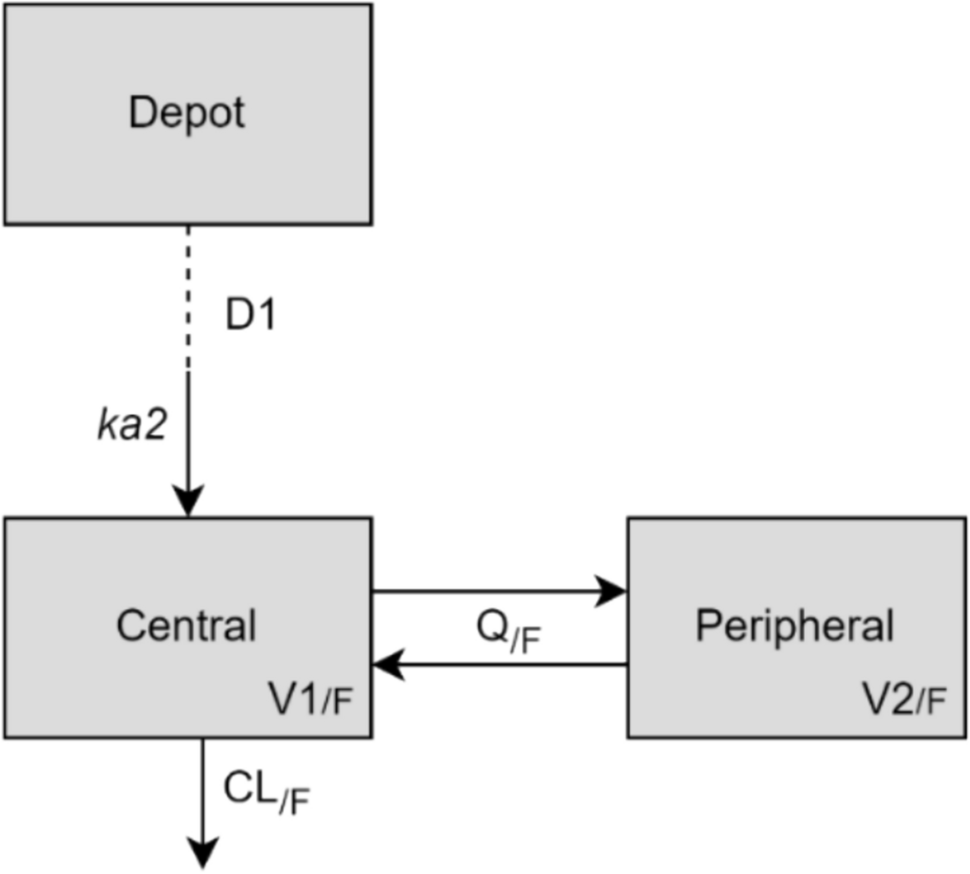
2.3.1 Base ModelGiven the limited data points available, a previously published model was refined to best describe our observations and accurately capture the pharmacokinetics of fexofenadine in this patient population [12]. A two-compartment model with sequential zero- and first-order absorption was employed, with linear elimination from the central compartment (Fig. 1). The dual absorption process was modeled with a zero-order absorption phase (duration D1), followed by a first-order absorption phase (rate constant ka2). Literature-sourced values for D1 and ka2 were 1.59 hours and 0.282 h⁻1, respectively [12].
Fig. 1
Compartmental model used to describe fexofenadine plasma concentration–time profiles. CL/F apparent clearance of fexofenadine, D1 duration of the zero-order absorption, ka2 rate constant of the first-order absorption, V1/F and V2/F apparent distribution volume of central and peripheral compartment, respectively, Q/F apparent inter-compartmental clearance
Our analysis aimed to investigate the impact of several covariates, such as age and renal clearance, on the variability in fexofenadine exposure. We incorporated interindividual variability (IIV) into the model, initially testing the variability in clearance (CL/F), the two volumes of distribution (V1/F and V2/F), and the absorption rate constant (ka), all using a log-normal distribution as in the original model. We then assessed whether our data supported the inclusion of these variabilities, ultimately retaining those that best described the observed variability in fexofenadine exposure. Additionally, several error models were evaluated to accurately capture the residual variability.
2.3.2 Covariate ModelThe relationships between pharmacokinetic parameters and plausible covariates, including demographic factors (e.g., body weight, age, gender), environmental influences (e.g., smoking status), and laboratory measurements (e.g., alanine aminotransferase [ALT], aspartate aminotransferase [AST], bilirubin, albumin, gamma-glutamyl transferase [GGT], alkaline phosphatase, creatinine clearance [CLcr] calculated using the Cockcroft-Gault equation, and urea), were evaluated. Additionally, drug use that could inhibit or induce Pgp activity was considered, categorized as no interaction, Pgp inhibitor, or Pgp inducer. Population type (pooled healthy volunteers vs hospitalized patients) was treated as a unique covariate to assess differences in drug pharmacokinetics between these groups.
To identify statistically significant covariates, a forward inclusion followed by backward deletion approach was employed, using either Eqs. 1 or 2:
$$}_= }_}}}_}}\right)}^^_}$$
(1)
where Pari and ηi are the individual (i) pharmacokinetic parameters and corresponding IIV element, respectively; β is the parameter capturing the continuous covariate (Cov) effect on the population parameter (Parpop), Covweight is Cov weighted mean or typical value in case of body weight (70 kg) and CLcr (100 mL/min);
where βj is the parameter for Covj, j is the component of the categorical covariate Cov, relative to the reference category, and the remaining terms are as previously defined.
Missing values in continuous covariates were imputed using the corresponding median values in the population of hospitalized patients or set to typical values of a healthy volunteer for missing laboratory values in this population, whereas missing values in categorical covariates were treated as a separate category.
2.3.3 Model Selection and EvaluationThe difference in importance sampling objective function values (ΔOFV, approximating a χ2 distribution) was used for model selection. A significance level of 0.05 was chosen for both base model development and forward/backward covariate selection steps. For non-nested models, the corrected Bayesian information criterion (ΔBICc) was used, retaining the candidate model if ΔBICc was less than − 2 compared with the reference model [13].
Additional model evaluation tools included visual inspection of goodness-of-fit (GOF) plots (e.g., observed vs predicted concentrations), the precision and plausibility of parameter estimates, and prediction-corrected visual prediction checks (pcVPCs) [14]. The latter allowed final model evaluation by comparing observed percentiles with model-based simulations (n = 500).
Nonparametric bootstrap analysis, implemented in the Rsmlx package, was used to assess the reliability of the final model. Pharmacokinetic parameters and variabilities were estimated for each resampled dataset (n = 1000), and original estimates were compared with the bootstrap median and 95% confidence interval (95% CI).
2.3.4 Model-Based SimulationsThe final model was used to simulate 1000 virtual subjects, stratified by chronic kidney disease (CKD) stage, age group, and the presence or absence of Pgp inhibition. CKD stages were defined as follows: stage 1 (CLcr > 90 mL/min), stage 2 (CLcr 60–89 mL/min), stage 3 (CLcr 30–59 mL/min), stage 4 (CLcr 15–29 mL/min), and stage 5 (CLcr < 15 mL/min). Age groups were stratified into 10-year intervals from 20–30 years to 90–100 years. For each combination, simulations were performed with and without a Pgp inhibitor.
The area under the concentration–time curve from 0 to 6 hours (AUC0–6) of fexofenadine was extracted for each group and compared with the AUC0–6 of a typical healthy volunteer (a 20-year-old with a CLcr of 100 mL/min and no Pgp-modulating medication), as established in the Bosilkovska et al. study [4]. Differences in AUC0–6 were expressed as ratios, facilitating the interpretation of the current categorizations for healthy volunteers, as shown in Table 1, adapted from Bosilkovska et al. [4].
Table 1 Characterization of Pgp activity based on AUC0–6 of fexofenadine adapted from Geneva cocktail study data [4]
留言 (0)