
記住我








446 of the 1028 patients (43.39% response rate) invited to the study completed the questionnaire. Exclusions were made for 157 patients due to incomplete responses, 48 due to diagnostic discrepancies (including benign conditions or sarcoma location criteria not met), and 4 due to missing treatment information, leaving 237 patients (mean age = 52 [17]; 104 females, 133 males) eligible for analysis. Reasons for non-participation included 27 deceased patients, 111 undelivered invitation letters, and 497 unresponsive invitees.
Not all participants underwent all treatments, whereas some patients had a combination of therapies. In total, we counted 94 patients for radiotherapy, 67 patients for chemotherapy and 225 patients for surgery.
The average age of all 237 participants was 52 years (range 18–93 years). Among the participants, 133 were male, and 104 were female, indicating a balanced distribution (see Table 1).
77.6% of all patients described their current situation as tumorfree and under surveillance. 3.8% stated to be under curative therapy and 7.2% were undergoing palliative therapy. 11.4% did not know or could not determine their situation clearly.
There were 45 different subtypes (some very similar were summarized) of STS included in the study. The four most common subtypes were leiomyosarcoma, dermatofibrosarcoma protuberans, alveolar sarcoma, and liposarcoma (see Table 1). It is important to note that patients were asked about their diagnoses, but in general their statements were not cross-checked with clinical data.
Frequency of modalitiesParticipants were asked about the number of therapy modalities they received. In addition to the three primary modalities of radiation, surgery, and chemotherapy, isolated limb perfusion (ILP) and hyperthermia were also considered. Among the participants, 108 received more than one therapy modality, while 129 underwent only one modality (Table 1).
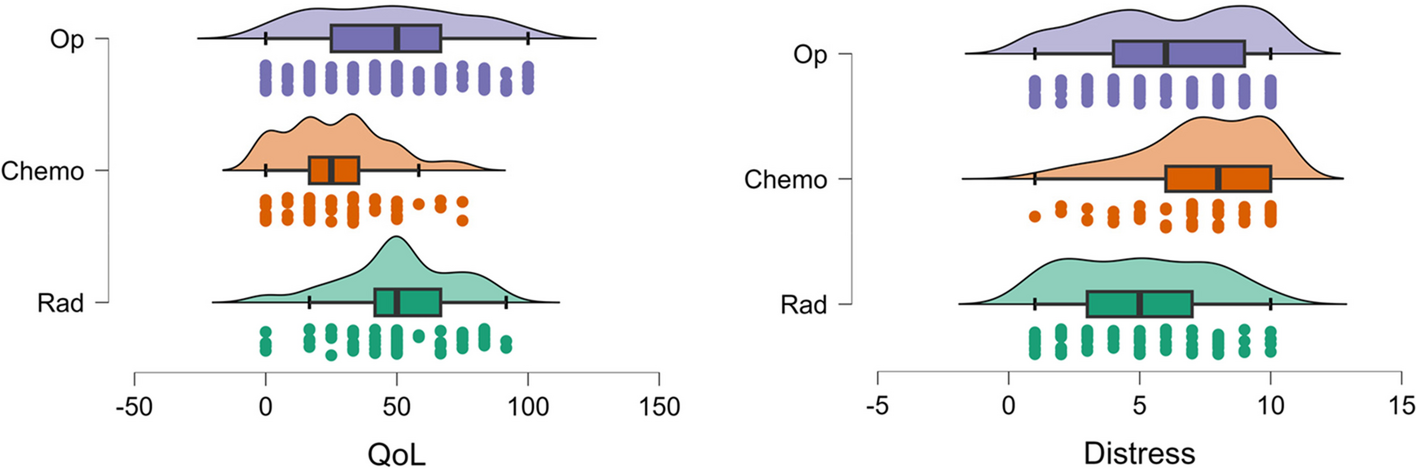
Distress, retake and quality of lifeDistressFigure 1 shows the mean difference in distress across different types of treatment. Participants reported the most distress for chemotherapy. We found a statistically significant difference in average distress according to treatment type (F (2, 169) = 18.306, p < 0.001, eta-squared = 0.07). A Tukey post-hoc test revealed significant pairwise differences between treatment types of radiation and chemotherapy with a mean difference of -2.408 (p < 0.001, d = -0.873), between radiation and surgery with a mean difference of -1.046 (p = 0.006, d = -0.379), and between chemotherapy and surgery with a mean difference of 1.362 (p < 0.001, d = 0.494).
Fig. 1
Mean distress scores for the three treatment types. Error bars visualise the 95% confidence interval
RetakeA chi-squared test was conducted to examine the relationship between retake and treatment modality. The results indicated a significant association, χ2 (2, N = 427) = 26.209, p < 0.001. Retreatment rates varied by treatment modality, with the highest percentage reported in the surgery group (94.19%), followed by radiotherapy (87.38%), and chemotherapy (73.49%).
Quality of lifeA statistically significant distinction was observed in terms of quality of life (F (2,183) = 31.96, p < 0.001, eta squared = 0.096). Subsequent Tukey post-hoc analysis revealed notable pairwise differences between treatment modalities. Specifically, there were significant differences between radiotherapy and chemotherapy, with a mean disparity of 24.1 (p < 0.001, d = 0.951), as well as between chemotherapy and surgery, with a mean difference of -20.05 (p < 0.001, d = -0.790). However, the discrepancy between radiotherapy and surgery, with a mean difference of 4.1, did not reach statistical significance (p = 0.389, d = 0.161).
EORTCA comparison is made among radiotherapy, chemotherapy, and surgery in terms of global health, functional scales, and symptom scales. Table 2 illustrates the mean difference between the three modalities, together with the p-value from the Tukey post-hoc test and Cohen’s d. Table 3 presents a one-way analysis of variance, with group sizes of n = 95 for radiation, n = 68 for chemotherapy, and n = 225 for surgery.
Table 2 Oneway analysis of variants: comparison of the means of all three different conditionsTable 3 Mean difference between modality groupsEORTC—functional scalesEncompassing physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning. Physical functioning was significantly highest during radiotherapy, with a mean score of 63.5 [25.6] (F (2,176) = 13.490, p < 0.001, eta squared = 0.050). In contrast, both operation (mean = 50.3 [32.8]) and chemotherapy (mean = 43.5 [25.4]) exhibited significantly lower scores, although they were not significantly different from each other. This pattern was also consistent for the other functional scales as well (except emotional functioning), with chemotherapy having a more pronounced effect on well-being, resulting in significantly lower scores compared to operation and chemotherapy. However, there were no significant differences between surgery and chemotherapy. The p values for emotional functioning indicated no significant difference between the three modalities. Detailed values for role functioning, emotional functioning, cognitive functioning, and social functioning can be found in Tables 2 and 3.
EORTC—symptom scalesNotably, when it came to pain (F (2,385) = 9.703, p < 0.001, eta squared = 0.048), surgery (mean = 50.1 [36.0]) was significantly more discomforting than radiotherapy (mean = 31.8 [32.5]) and chemotherapy (mean = 40.9 [32.6]). However, radiation and chemotherapy did not exhibit a significant difference (Table 3).
Insomnia and sleep disturbances (F (2,164) = 5.813, p < 0.001, eta squared = 0.027) were reported predominantly during chemotherapy, with a mean score of 51.5 [36.8]. This score was significantly higher compared to radiation, which had a mean score of 33.0 [33.2]. There were no significant differences between surgery (mean = 39.7 [37.6) and chemotherapy in this regard.
Nausea and vomiting (F (2,385) = 41.473, p < 0.001, eta squared = 0.177) were primarily associated with chemotherapy (mean = 41.2.0 [36.5), while the values for radiation (mean = 12.5 [21.2]) and surgery (mean = 10.4 [21.8]) were significantly lower.
Regarding symptom scales related to fatigue, dyspnoea, appetite loss, constipation, and diarrhoea, a pattern similar to that seen in some of the functional scales mentioned earlier emerged. Chemotherapy resulted in significantly higher symptom scores compared to radiotherapy and operation, which did not exhibit significant differences between them.
Financial difficulties (F (2,151) = 2.346, p 0.099, eta squared = 0.013) were reported at a similar level across all three modalities, with no significant differences detected in the values of this scale.
留言 (0)