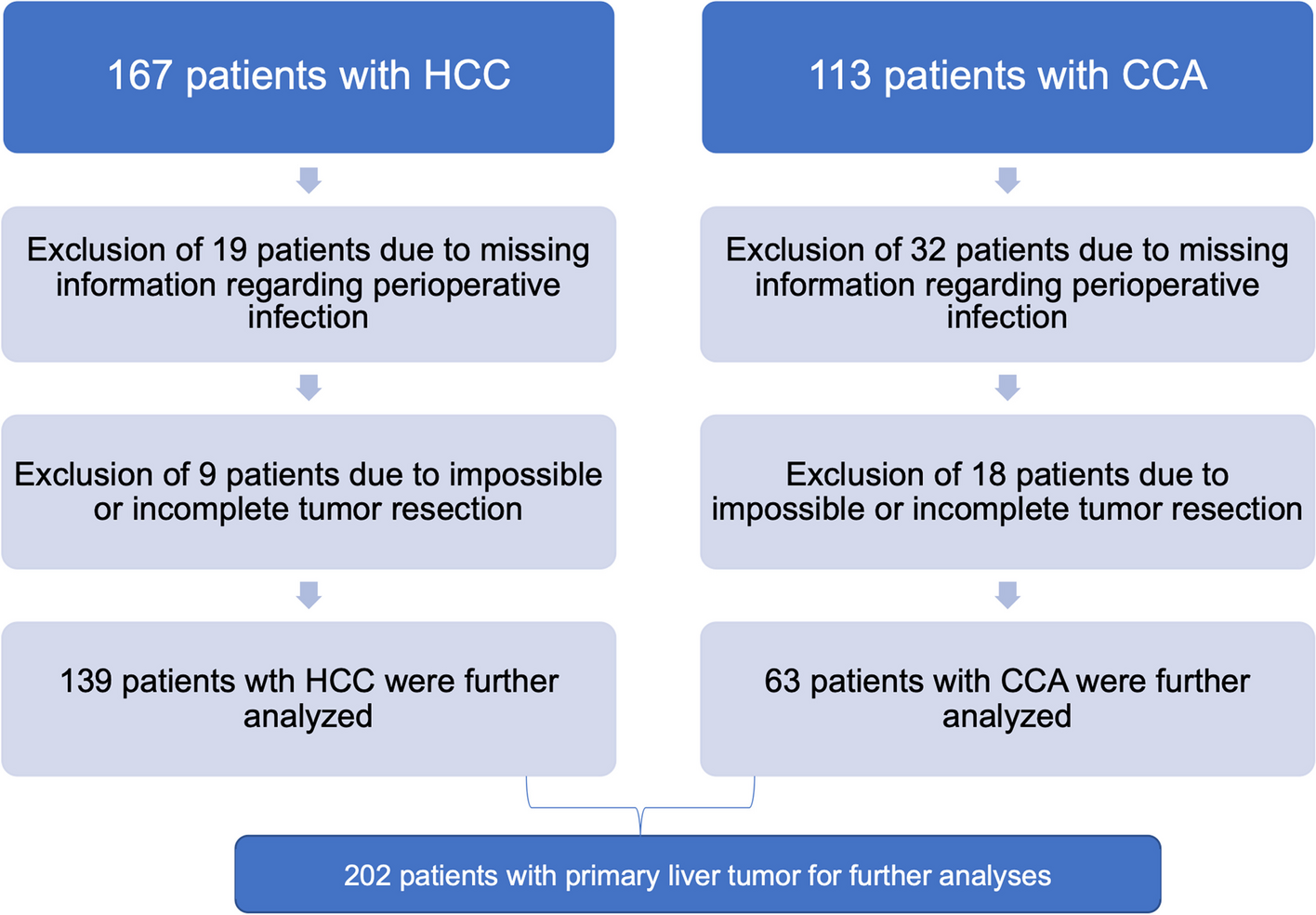
In this retrospective study, we analysed the impact of perioperative infections on overall survival in 202 patients who underwent liver surgery for primary liver cancer (HCC and CCA). Patients with perioperative infection had significantly worse overall survival compared with patients without clinically apparent infection. Strikingly, subgroup analyses showed that this observation was only true for patients with HCC, but not for those with CCA. Furthermore, patients with HCC who underwent limited liver resection had a better OS compared to patients who underwent hemihepatectomy.
Liver cirrhosis represents the most important risk factor for HCC but has only a relatively weak association with the development of CCA. In line, 73.4% of our patients with HCC had concomitant liver cirrhosis, while only 22.2% of CCA developed within a cirrhotic liver. Since an impaired liver function represent a major risk factor for an unfavorable clinical course in patients with infectious diseases, we hypothesized that the different effect of perioperative overall survival in patients with HCC and CCA might partially be due to the different frequencies of liver cirrhosis in the different sub-cohorts (HCC or CCA) of this study [12]. Interestingly, Kaplan–Meier curve analyses revealed that the main difference in survival occurs within the first weeks after surgery, while at later time points, the curves run parallel to each other, arguing for the need of optimal patient selection and preparation before surgery. We therefor hypothesize that any perioperative infections are an important predictor for short term postoperative survival especially in patients with HCC. Whether further immunological factors triggered by the perioperative infection might play a role in determining the patients´ survival in the long-run cannot be determined by our retrospective data analysis.
The imminent danger of infections in patients with liver cirrhosis is well studied [12]. Patients with cirrhosis are at increased risk for bacterial infections and the mortality of these patients is increased fourfold compared to patients without cirrhosis [13,14,15]. In cirrhotic patients, the immune system is deficient, but constantly active at the same time [12]. Both innate and adaptive immune response are affected, including monocytes, T-cells and B-cell, providing a mechanistic base for the effects observed in our analyses [16, 17]. As a consequence, our data stress for a strict surveillance of infections in cirrhotic patients, especially in the context of liver surgery, to avoid elevated mortality. Of interest, liver cirrhosis itself had no impact on survival in our cohort nor in the subgroups (Supplemental Fig. 1A-C), indicating that combination of impaired immune system due to cirrhosis and additional acute infection might be a necessity for our findings.
Moreover, we identified in patents with HCC, that non-anatomical tumor resection and therefor tissue sparing surgery had a positive effect on overall survival. Interestingly extend of surgery had no effect on OS in patients with CCA. This might again be related to the higher number of patients with preexisting liver cirrhosis in the group of HCC patients, although as stated before cirrhosis had no independent influence on OS in our cohort. However, it should be highlighted that all patients were carefully screened before surgery and it was ensured that the remaining liver function after surgery was sufficient. This probably explains why liver function based on the CHILD stage alone was not a decisive factor in our cohort. It should also be noted that extended liver surgery is often associated with larger or less favorably located liver tumors, which could also explain the difference in survival in HCC. In general, after surgery on a cirrhotic liver, at least about 40% of the liver tissue needs to be preserved [18] and our data support non-anatomical- parenchyma sparing- resections at least in HCC patients if possible [19,20,21,22].
Furthermore, our data suggest a better OS for patients with chronic viral hepatitis B or C, independent of perioperative infection. Previous studies demonstrated a comparable OS for viral and ALD triggered HCC [23]. However, in our cohort an influence of the ongoing viral infection and potential concomitant immunological effects on OS is possible. Chronic viral infections are a common cause of cirrhosis and HCC. The immune response following viral infection may have a relevant impact on liver-derived tumors, which has been extensively studied in HCC [24]. Interestingly, this observation matches data from several recent treatment studies for liver tumors, which also indicated better treatment success in patients with underlying viral hepatitis B or C [25]. Whether the improved survival of patients with viral hepatitis in our cohort is also related to immunological processes or due to other confounders, cannot be conclusively clarified with the present data. However, the immunological differences between viral and non-viral HCC demonstrate the relevant influence of the immune system on the tumor disease and thus survival in a postoperative setting.
The data presented here highlight the role of perioperative infections as a important parameter in patients with HCC (but not with CCA) for at least short term survival and further endorse the role of liver cirrhosis as a risk factor in patients receiving (major) liver surgery. Furthermore, tissue sparing liver resection in patients with HCC seem to improve long term survival. Nevertheless, our analyses face important limitations, which are due to the study design and cannot be avoided. First, our study included only 202 patients, representing a limited cohort of patients when analyzing complex endpoints such as overall survival. Second, our study represents a retrospective analysis conducted at a single center only, thus center-specific bias cannot be excluded. Due to the retrospective format data collection is often incomplete and important potential confounders as severity of liver disease, comorbidities, and perioperative care practices can’t be always reflected in detail. Additionally, patients were included over a long period of time during which the assessment of infections as well as operation techniques might have changed. Especially perioperative management and infection prevention has undergone changes over this long period of time, generally infection control is supposed to have improved, but multi-resistant bacteria are emerging as well and complication treatment. Moreover, postoperative increase in markers for inflammation like CRP is common as well as detection of bacteria in intraoperative bile samples. Therefor misclassification of “infection” is a possible confounder, even by using only a combination of increased inflammation markers and pathogen detection for defining “infection”. In addition, patients with two different tumor entities were included. Furthermore, our study cannot distinguish whether it is really the extent of the surgical resection or the size of the liver tumor that necessitated the extensive resection that is responsible for the differences in overall survival. Finally, our data does not provide evidence on whether an individual patient might have benefitted similarly or even more in terms of long-term survival, from a different treatment modality such as systemic treatment or other locally ablative therapies. This important clinical question can only be answered by further prospective clinical studies including different treatment modalities and providing a streamlined treatment protocol avoiding bias due to incomplete data collection and treatment changes over time as stated before. Such studies would not only improve the clinical management of patients with liver cancer but could also provide important insights into the pathophysiology of HCC (and CCA) if appropriate translational programs are integrated into the respective study-design. We hope that in the long term this study will help to improve the perioperative management of patients with liver tumors and encourage those needed further prospective studies, particularly to improve infection control in this patient group.









留言 (0)