
記住我

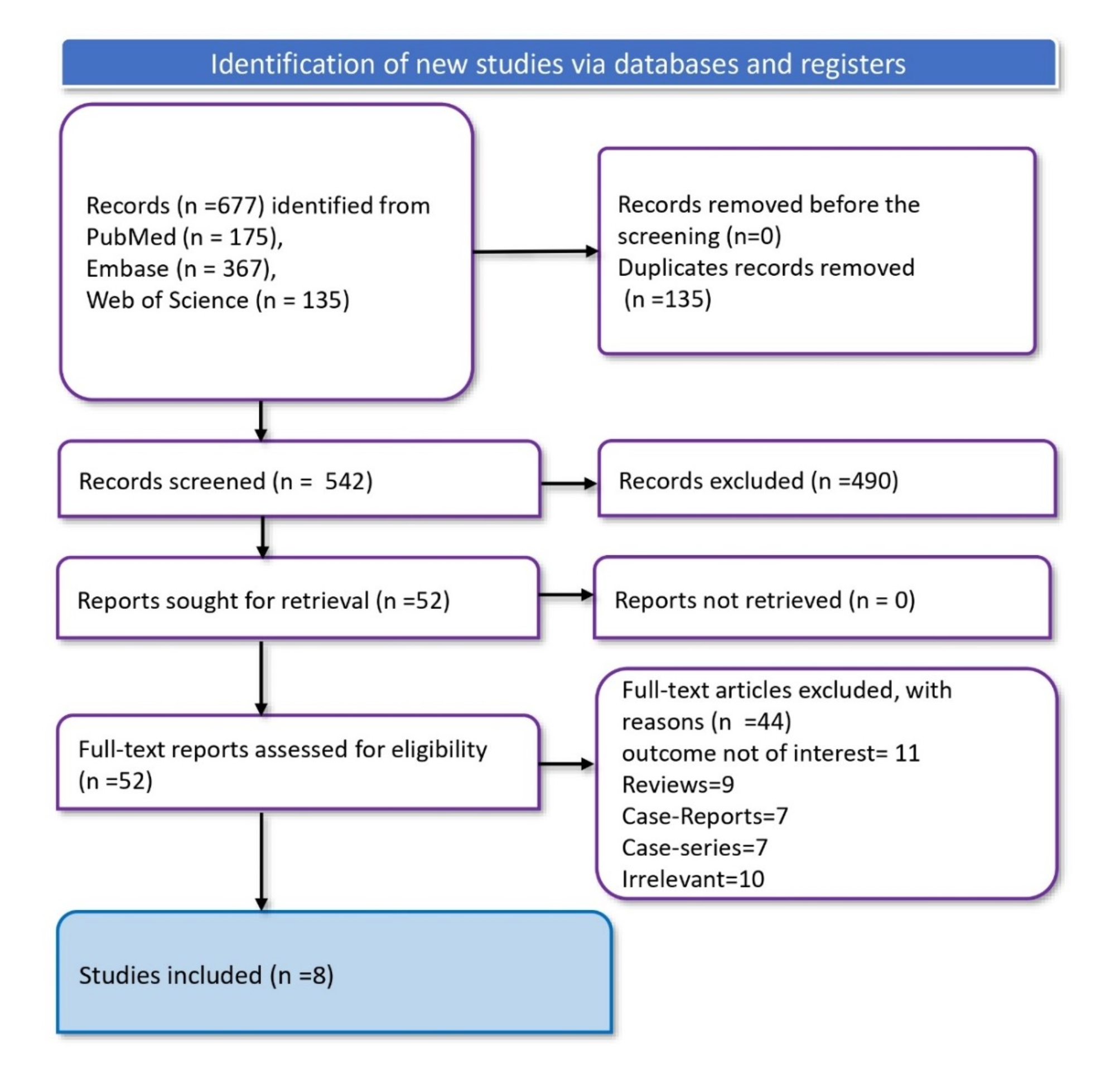


Based on prespecified inclusion and exclusion criteria, we selected 190 patients who developed forearm hematomas following transradial coronary intervention (TRI) at our hospital from March 2021 to March 2023. Using a random number table method, the patients were divided into two groups: the research group (95 cases) and the control group (95 cases). The study protocol received ethical approval from the hospital ethics committee. and all 190 patients provided informed consent. One patient from the control group withdrew due to discomfort during cuff compression, leaving 189 patients who successfully completed the study (Fig. 1).
Fig. 1
Design of innovative device
The inclusion criteria were as follows: (1) Aged between 18 and 75 years; (2) Meeting diagnostic criteria for coronary heart disease; (3) Hematoma area ≥ 50 mm × 50 mm; (4) Tolerance to both thermostatic ice and cuff compression; (5) Systolic blood pressure < 150 mmHg; and (6) Normal coagulation parameters. Exclusion criteria included: (1) Speech impairment; (2) Intravenous administration of GP IIb/IIIa receptor blockers; (3) Forearm trauma or arteriovenous fistula; (4) Contraindications to cold therapy; and (5) Occurrence of vagal reflexes during thermostatic ice application and compression.
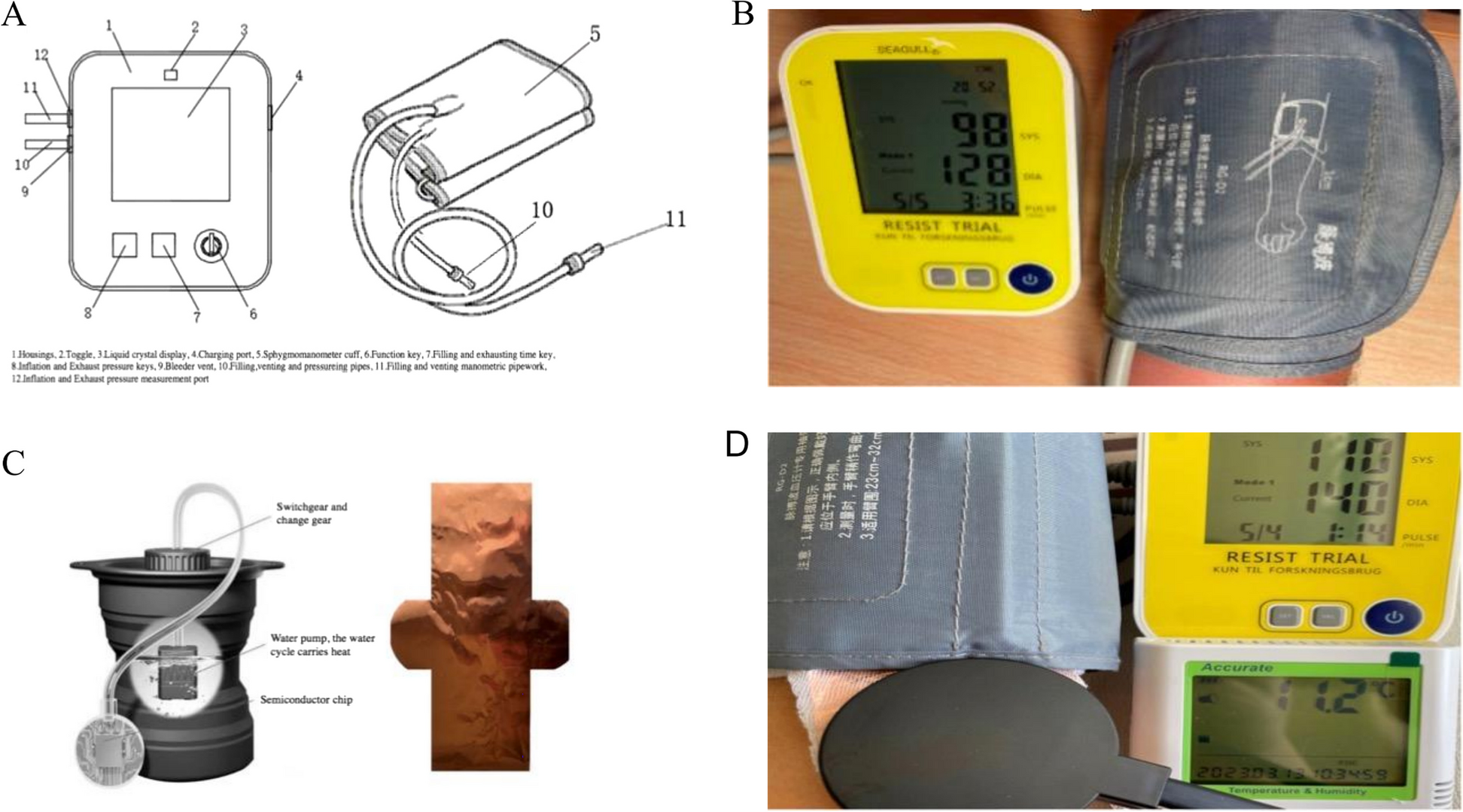
Design of innovative deviceThe innovative device used in this study comprised two key components: a multifunctional pulse wave sphygmomanometer and a thermostatic ice application device.
Multifunctional pulse wave sphygmomanometer: This device includes a Bluetooth-enabled chip for user control via a dedicated app, allowing customization of cuff inflation and deflation cycles, pressure levels, and timing. It features dual pumps, dual sensors, and dual tubing with separate inflation and exhaust tubes for precise pressure management. The device also supports programmable one-touch operation with a Start/Pause button (Fig. 2).
Fig. 2
Thermostatic ice application device: This device is made of a 10 μm ultra-thin, highly flexible copper material with excellent thermal conductivity. The copper, housed in a gauze sleeve, aligns with the cuff’s width and interfaces with a custom water-cooled semiconductor cooling radiator. The radiators connect to the protruding ends of the purple copper, and foam dressing on the skin-facing side prevents frostbite. A semiconductor refrigeration chip and water pump control the temperature control, maintaining a stabilized range of 10℃ to 15℃ on the forearm surface during icing (Fig. 2).
Management of forearm hematoma in control groupFor the control group, a nurse measured brachial blood pressure using the custom-designed multifunctional pulse wave sphygmomanometer. After pressing the pause button, the cuff was affixed to the most swollen portion of the forearm and the procedure was initiated by pressing the start button. The sphygmomanometer, pre-programmed with factory-customized parameters, ensured consistency.
The cuff inflated to a pressure 30 mmHg above the systolic level for 5 min then deflated to the diastolic pressure for 1 min. This compression-decompression cycle was repeated approximately five times. The device maintained the specified constant pressure throughout the process.
Management of forearm hematoma in research groupIn addition to the control group’s procedures, the research group integrated thermostatic ice application. After measuring arm circumference and blood pressure, a nurse placed a 10 μm-thick copper strip, housed in a gauze sleeve, around the forearm. This assemblage was then gently secured around the forearm, centered at the designated mark, for a duration of one week. Subsequently, the cuff was affixed to the surface of the purple copper, and the two protruding ends of the copper were connected to a custom water-cooled semiconductor refrigeration radiator.
The protocol for cuff compression was identical to that of the control group but included simultaneous thermostatic ice treatment. Blood pressure and heart rate were monitored, and interventions ceased if patients could not tolerate the treatments.
Endpoints, definitions, and quality controlEndpointsThe primary endpoint was the effective rate of one compression. Other endpoints included body surface temperature, pain, comfort, arm measurements, and swelling value.
Definitions Body surface temperatureMeasured with the Hua Hanwei T40W-PT body thermometer, ensuring uniformity within the same batch. The measurement accuracy was maintained at 0.1℃.
PainAssessed using the pain numeric rating scale and the visual analogue scoring method, ranging from 0 (no pain) to 10 (severe pain) [9]. Mild, moderate, and severe pain were categorized between scores 1–3, 4–6, and 7–9, respectively.
ComfortClassified into three levels: Level 1 represented forearm or palm swelling without pain; Level 2 denoted swelling and bearable pain; and Level 3 signified intolerable swelling and pain.
Effective rate of one compressionCalculated as the ratio of individuals displaying no blood extravasation from the swelling, as suggested by vascular ultrasound after five cycles of forearm hematoma cuff compression. The effective rate of primary compression was calculated as (number of individuals without blood extravasation / total number of individuals in each group) × 100%.
Arm measurementsForearm circumference at the maximum swelling point and the same site on the healthy side, measured using the GemRed electronic display soft tape with 1 mm precision.
Swelling valueCalculated by subtracting the arm circumference at the most swollen point of the forearm from the healthy arm circumference.
Quality controlA 14-member intervention team with an average of 13.54 ± 3.23 years of professional experience was assembled. The team included two medical doctors with expertise in post-compression vascular ultrasound, two seasoned provincial cardiovascular specialist nurses for guidance and quality control, and 10 senior charge nurses for patient recruitment and intervention.
Multiple rounds of comprehensive training were provided, including proficiency in the operation and maintenance of the custom-designed multifunctional pulse wave sphygmomanometers and the self-crafted thermostatic ice packs. Equally, they received training in the collection of pertinent evaluation indicators to enable competent execution of the tasks. Prompt action was taken upon identifying a forearm hematoma in patients post-TRI surgery. Two team-member nurses expeditiously measured and annotated the forearm’s circumference at its most swollen point. Following this, cuff compression and/or thermostatic ice application were promptly administered to the forearm hematoma. This approach aimed to ensure both the effectiveness of the intervention and the precision of indicator parameter measurements.
Statistical analysisAll statistical analyses were conducted using SPSS 25.0. Quantitative data with normal distribution are presented as mean ± standard deviation and analyzed using the independent samples t-test. Data not conforming to a normal distribution are expressed as median and quartiles. Qualitative data are presented as frequency (%) and analyzed using the chi-squared X2-test. A significance level of α = 0.05 was employed for all tests.
留言 (0)