At present, it is widely recognized that the occurrence and development of CHD are the result of the combined effects of multiple associated risk factors, and abnormal lipid metabolism is now recognized as the most important risk factor for CHD [19]. Non-HDL-C, which is equivalent to the sum of celiac disease, very low-density lipoprotein, intermediate-density lipoprotein, LDL-C, Lp(a), and other lipoprotein particles, were included in this study [20], which is one of the first indicators of lipid management currently recommended as a good indicator of the extent of vascular disease [21]. Rutger et al. evidence supports the claim that non-HDL-C is superior to LDL-C in Cardiovascular disease (CVD) risk estimation [22, 23]. Our findings also suggest that Non-HDL-C is superior to LDL-C in terms of value in assessing coronary heart disease risk. Regression analysis showed that Non-HDL-C was an independent risk factor for CHD, and Non-HDL-C was also significantly correlated with the degree of stenosis of CHD in correlation analysis. A considerable number of studies have shown that there are different degrees of correlation between IR and atherosclerosis and that individuals at high risk of cardiovascular events can be detected at an early stage by using the TyG index, which is a significant risk factor for CVD [24,25,26]. Lipid metabolism and glucose metabolism can interact with each other and lead to the occurrence of cardiovascular events [27]. However, no study has been reported on the combination of TyG index and Non-HDL-C for the prediction of coronary heart disease. Therefore, the present study was conducted to investigate the predictive value of the combination of the above indexes for the occurrence of coronary heart disease.
The results of the present study showed that the percentage of males, history of diabetes, and history of hypertension in the CHD group was higher than that in the NCHD group, and the WBC, UA, TG, TC, LDL-C, Non-HDL-C, FPG, Cr, HbA1c, and TyG index in the coronary group were higher than those in the non-coronary group, suggesting that abnormalities of lipid and glucose metabolism, vascular sclerosis, and inflammation play an important role in the progression of coronary atherosclerosis. Further multifactorial regression analysis showed that sex, history of hypertension, HbA1c, Non-HDL-C, and elevated TyG index were independent risk factors for the development of coronary heart disease, and it was found that history of diabetes, WBC, Hs-CRP, LDL-C, Non-HDL-C, and TyG index was positively correlated with the Gensini score (P < 0.05), and sex was negatively correlated with the Gensini score (P < 0.05), suggesting that Non-HDL-C, TyG index is a reliable predictor of the occurrence as well as severity of coronary heart disease. 2023 Shin Young Yun et al.’ [28] study concluded that ApoB, Non-HDL-C, and LDL-C are independent risk factors for Atherosclerotic Cardiovascular Disease (ASCVD). In addition, most scholars believe that Non-HDL-C does not need to be measured separately, that its calculation is not affected by TG, and that fasting is not a necessary condition for testing [29]. The ease of calculation and the absence of additional costs make Non-HDL-C more useful than other lipid indices. Non-HDL-C has the advantages of easy calculation, low economic cost, and can be used for early diagnosis and prevention of coronary heart disease.
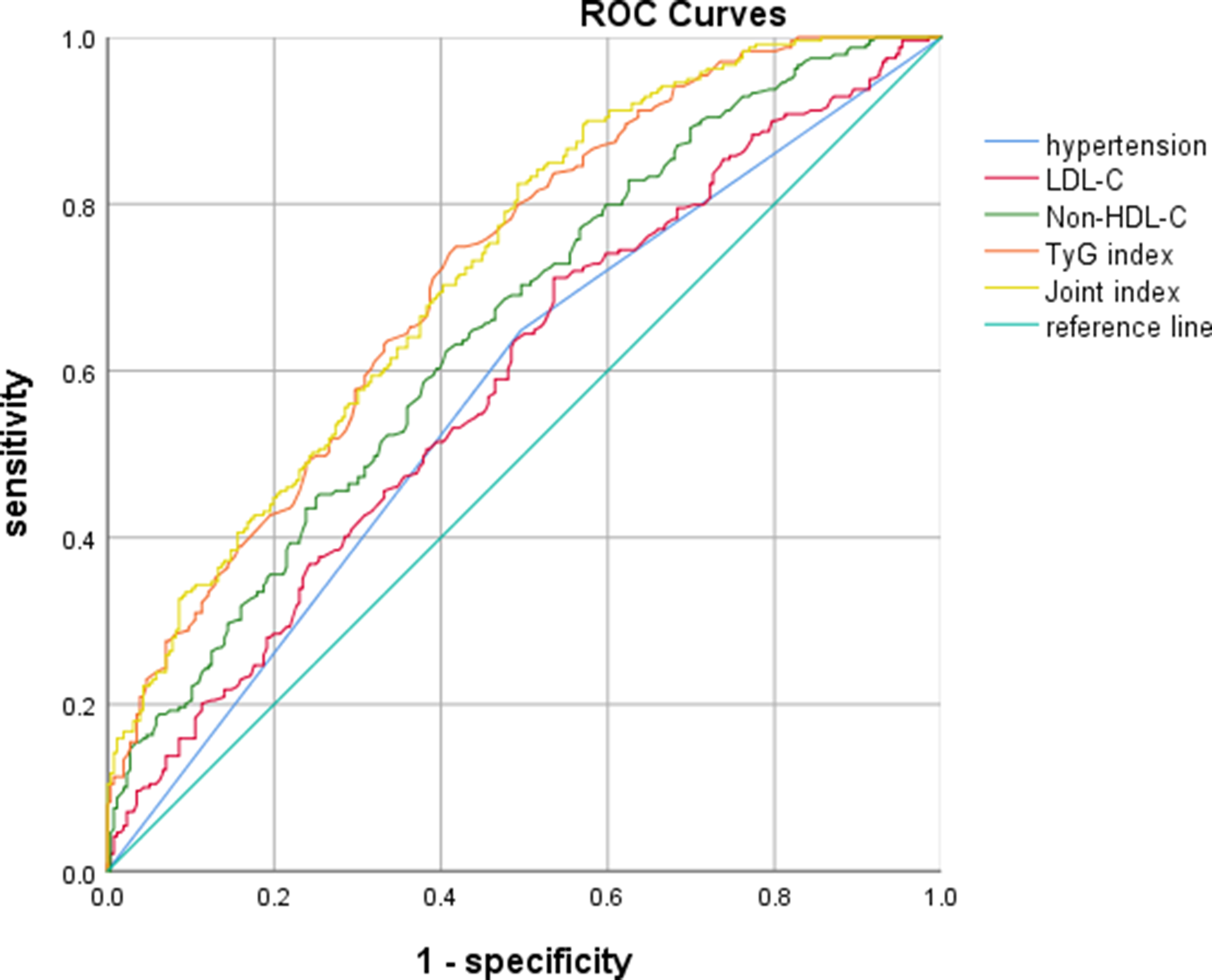
The TyG index was initially proposed as an index for evaluating IR, and studies have shown that one of the main relative risk factors for the onset of atherosclerosis includes IR, which reduces vasodilatation compared with the previous one and accelerates the rate of atherosclerosis [30, 31]. At present, a considerable number of studies have demonstrated various degrees of correlation between IR and atherosclerosis. In a Korean study that included 12,326 asymptomatic adults, the TyG index was shown to be an independent predictor of the progression of coronary artery calcification, especially in adults without severe coronary artery calcification [32], whereas coronary artery calcification is a valid marker of ASCVD and predicts adverse cardiovascular performance [33]. The study by Wang et al. also suggests that the TyG index may be a useful marker for risk stratification and prognosis in patients with ACS [34].In the present study, it was also shown that the TyG index not only has a high predictive value in the development of coronary heart disease but also has a high correlation with the degree of coronary artery stenosis. Our study also proved that TyG index has a higher diagnostic value (AUC:0.719) and can be used as a marker to predict the risk of coronary heart disease. Hypertension is also an important risk factor for the development of coronary atherosclerosis. Blood pressure at a high level for a long time will cause damage to the endothelial function of blood vessels, and under the action of vasoactive substances, causing left ventricular hypertrophy, atherosclerosis arrhythmia, and other symptoms, thus causing the occurrence of coronary heart disease [35, 36]. Research has shown that hypertension is easily combined with metabolic diseases such as obesity, abnormal blood glucose, and dyslipidemia and these metabolic diseases are also important reasons for the occurrence and development of cardiovascular diseases [37, 38]. Combined with the results of the present study, the high proportion of patients with coronary heart disease who had a history of hypertension and the higher Non-HDL-C and TyG indices in such patients suggest that early identification of different metabolic abnormalities in hypertensive patients is important for the risk of coronary heart disease in the hypertensive population.
There are some limitations in this study, firstly, this is a retrospective study, and the collection of clinical data may be biased. For example, there is a lack of inquiry about blood pressure and glycaemic control in the history of hypertension and diabetes, which may lead to bias in the predictive value of hypertension and diabetes as risk factors for coronary heart disease. Secondly, this study only included the data of patients in one hospital, however, the metabolic level varies in different regions and countries, and it is not clear whether our findings can be generalized to other ethnicities. Thirdly, Our study population is relatively small, and a longer study population should be included to obtain more convincing data. Finally, HOMA-IR was not analyzed and compared with TyG index because insulin levels were not measured in the general health checkup. In the future, large multicenter prospective studies should be conducted to further demonstrate the potential clinical value of Non-HDL-C and TyG indices in the prediction of coronary heart disease and coronary stenosis, taking into account the many factors that may affect these indices.




留言 (0)