Our case series highlights two patients diagnosed with pancreatic cancer (PC) following an episode of acute pancreatitis (AP). It is not uncommon for PC to be preceded by AP, with up to 5.9% of PC cases in the United States presenting similarly [2]. The mechanism behind this association is often attributed to pancreatic duct obstruction induced by the tumor, although various other correlations exist, contributing to the long-term impact of AP on PC formation [2, 7]. Generally, PC diagnosed after an AP episode carries a more favorable prognosis due to early stage detection and increased chances of surgical resection [2, 6]. However, our cases revealed diagnostic challenges that could potentially delay PC detection.
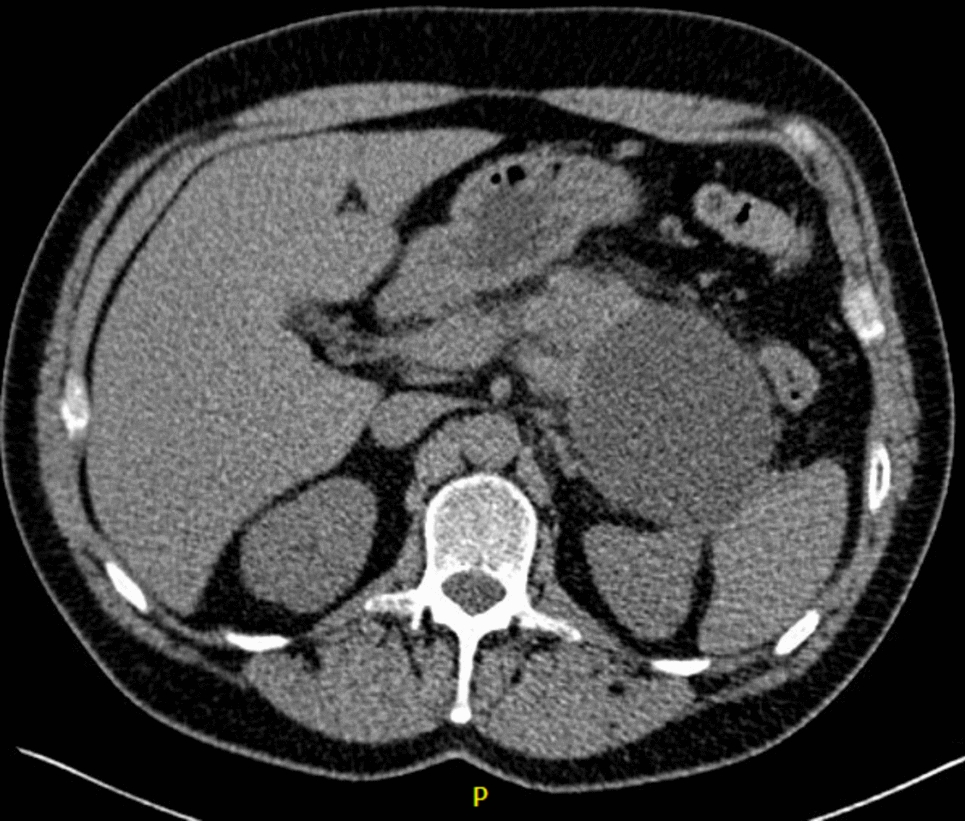
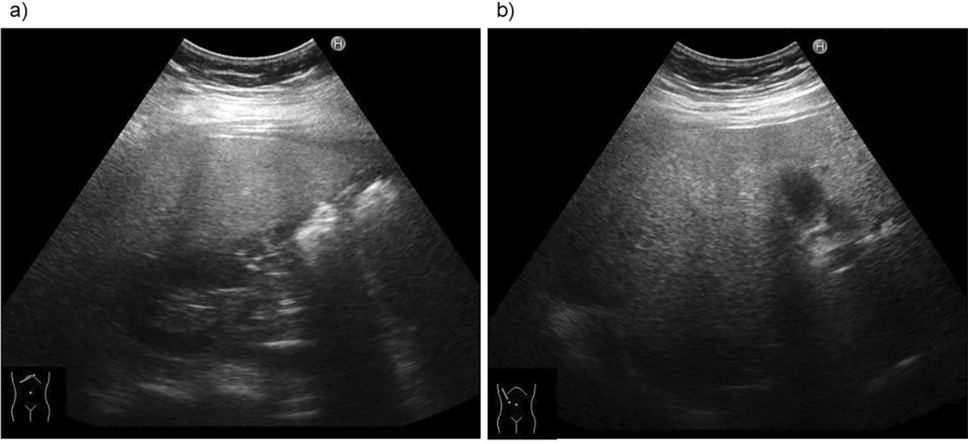
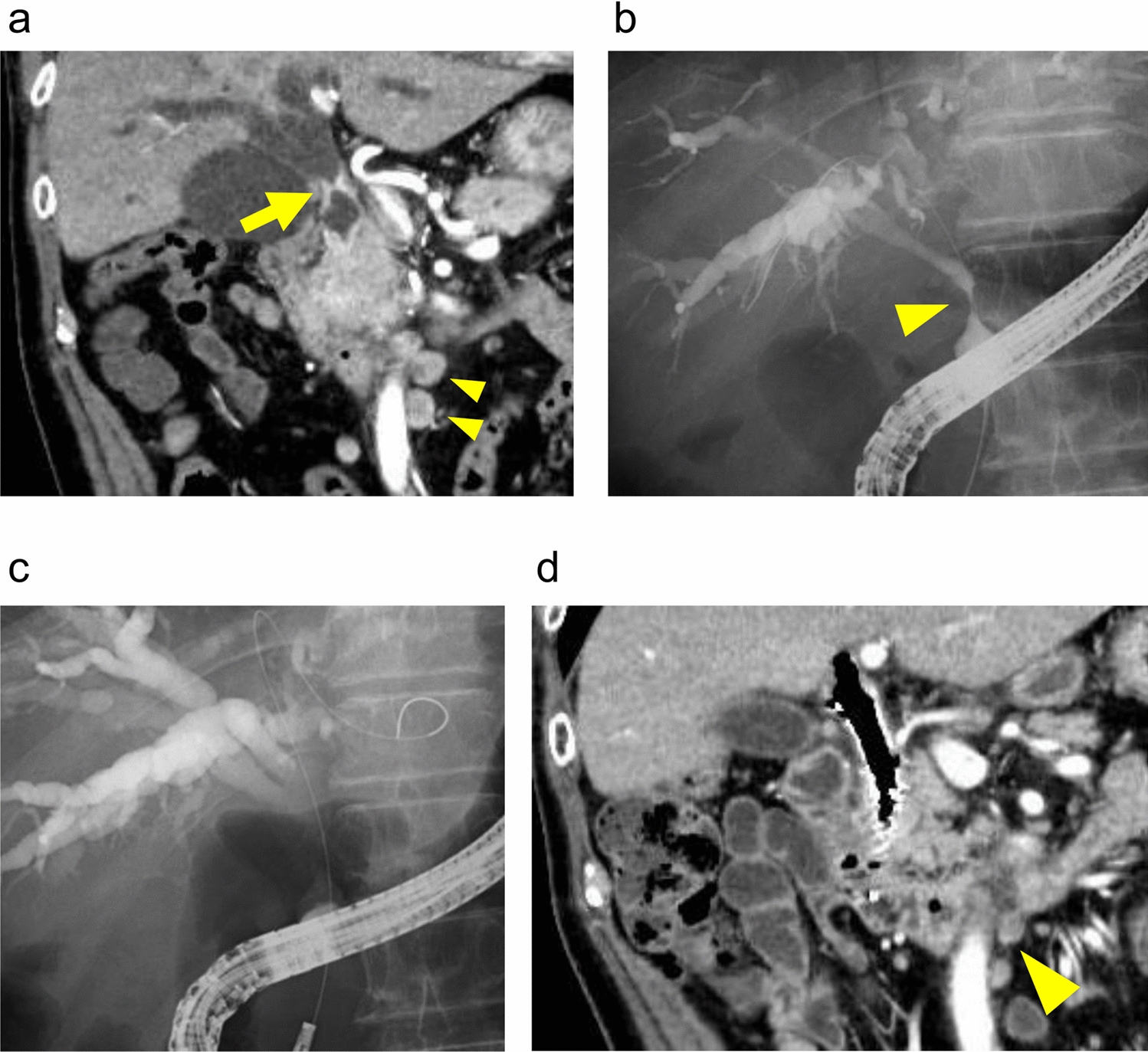
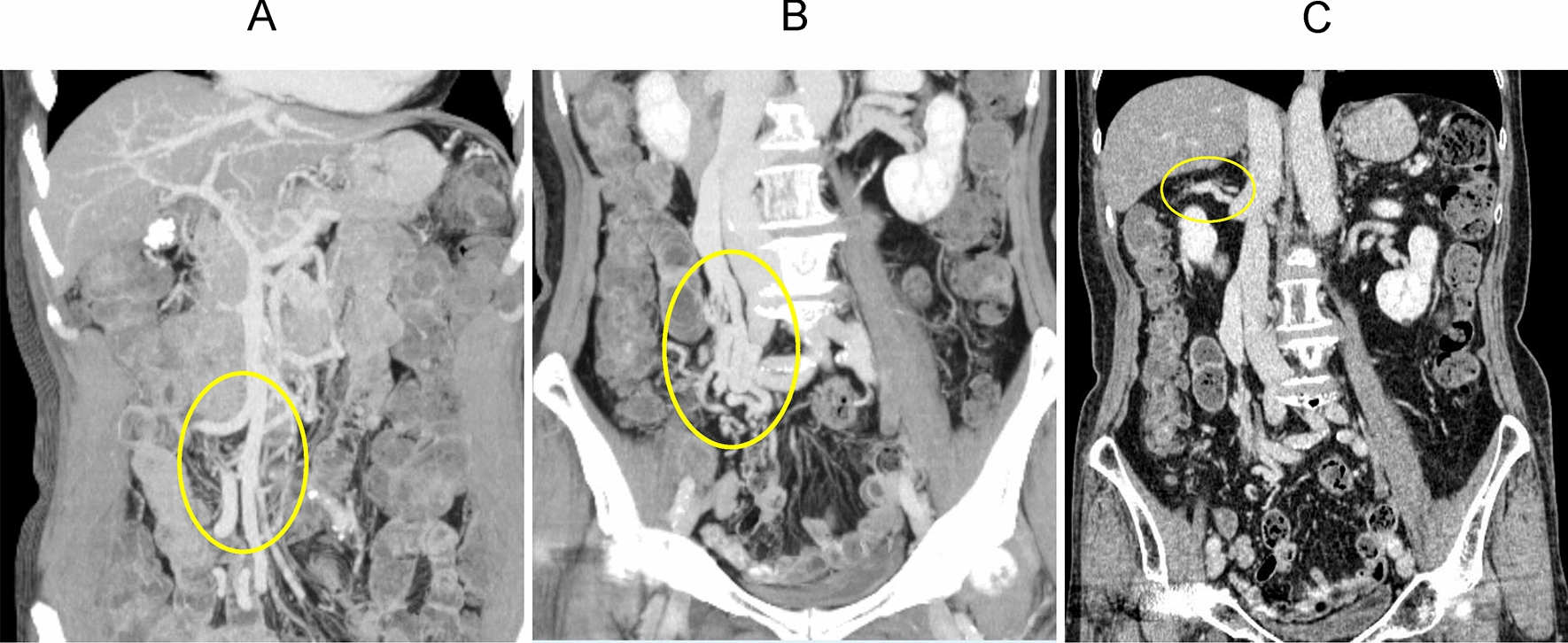
Following an episode of acute pancreatitis, as observed in our series, we noted peripancreatic fluid collection, which obscured the underlying tissue in conventional imaging. In addition, residual inflammation can limit the assessment of pancreatic tissue [8]. While it is reasonable to await the resolution of inflammation before delving into the etiology of pancreatitis, the spontaneous resolution of peripancreatic fluid collection may be prolonged. This delay could potentially mask or hinder the diagnosis of malignancy, particularly in the case of small, poorly enhancing solid tumors [9].
Providers may encounter cysts after an episode of acute pancreatitis, prompting questions about whether the cyst is a true pancreatic cyst, cystic degeneration of a pancreatic tumor, or wall formation following acute peripancreatic fluid collection [10]. Thus, even when patients exhibit typical pseudocyst imaging criteria, malignancy cannot be definitively excluded. In a surgical review involving 122 patients treated surgically for a pancreatic pseudocyst, 5 of them revealed cancer during the operation [11], and in a retrospective review of pseudocysts, 44% received a final diagnosis of pancreatic cystic neoplastic growth [12].
The probability of developing PC following an episode of acute pancreatitis (AP) is highest among elderly individuals, those with new-onset diabetes, individuals lacking a history of alcohol or biliary etiology, and those experiencing new-onset chronic pancreatitis [2, 13]. The first case highlights an additional diagnostic challenge posed by chronic pancreatitis, as it presents similar clinical manifestations to PC, such as weight loss, abdominal pain, and jaundice. Moreover, imaging may be constrained due to calcifications and inflammatory fluid collections associated with chronic pancreatitis [14]. Given it is crucial for early diagnosis of pancreatic cancer after the onset of AP, the literature suggests scheduled imaging within 3 months after discharge, such as CT or EUS. A follow-up CT within 3 months after discharge is beneficial, especially for patients with higher severity scores (CTSI ≥ 3) [15]. An unexplained acute distal pancreatitis is associated with an increased frequency of subsequent pancreatic cancer particularly pancreatic ductal adenocarcinoma resulting from obstruction of pancreatic duct by the tumor itself, and hence, the suggestion for EUS-guided biopsy should be considered in these patients on follow-up [16].
In cases of diagnostic challenges for possible pancreatic neoplastic growth, the most advantageous method is performing endoscopic ultrasound (EUS) for close pancreatic examination and tissue acquisition. Further molecular and histological investigation on EUS-obtained samples can help clarify the diagnosis [14]. However, conflicting results may arise between imaging and tissue analysis, necessitating a high index of suspicion for a diagnosis and possibly repeated EUS, despite its invasive nature. On the contrary, contrast-enhanced EUS (CE-EUS) has been shown to be effective in the diagnosis of pancreatic tumors, including those with cystic degeneration. One such study demonstrated a significant improvement in diagnostic yield for focal pancreatic lesions, increasing accuracy from 64% with unenhanced EUS to 91% with CE-EUS. This is particularly more evident in differentiation of cystic lesions, in which CE-EUS had a diagnostic yield of 96% compared to 71% with unenhanced [17].
Cystic degeneration in neuroendocrine tumors in pancreas varies across different studies and although this can occur in patients with pancreatic NETs, it s uncommon. Across different studies, around 10–18% of patients with pancreatic neuroendocrine tumors are associated with cystic degeneration [18].
Although most cases of PC stem from ductal origins, it is important to note that pancreatic adenocarcinoma is not the sole malignancy linked to AP. Our second case illustrates that neuroendocrine neoplasms can infrequently manifest as AP and can pose a diagnostic challenge due to post-AP alterations [19].
In conclusion, our case underscores the complex challenges involved in managing patients with concurrent pancreatic fluid collections, pancreatitis, and pancreatic adenocarcinoma. First, the association between chronic pancreatitis and an increased risk of pancreatic adenocarcinoma is complicated by the potential masking effect of calcifications and fluid collections. Second, the interpretation of imaging findings and cyst fluid characteristics can present conflicting information, as exemplified in our patient’s case where typical benign pseudocyst indicators conflicted with elevated CEA levels suggesting a mucin-producing cyst. In addition, both chronic pancreatitis and pancreatic cancer contribute to malnutrition and weight loss, further complicating the clinical picture. Lastly, while endoscopic ultrasound (EUS) stands out as the most accurate imaging test for identifying pancreatic cancer and enables tissue diagnosis, its invasive nature limits the frequency of serial examinations. These multifaceted challenges underscore the need for a comprehensive and nuanced approach to the care of patients with such complex and overlapping conditions.



留言 (0)