This retrospective analysis included aSAH patients classified as WFNS grades 4–5, defined as PGASH. These patients were admitted between January 2003 and June 2016, with WFNS assessments conducted at the time of admission. The study received approval from the Institutional Review Board (Ethik-Kommission, Medizinische Fakultät der Universität Duisburg-Essen; Approval No. 15–6331-BO) and was registered with the German Clinical Trials Register (DRKS; ID DRKS00008749). WFNS assessments were conducted upon patient admission. All procedures were performed in accordance with relevant guidelines and regulations, and informed consent was obtained from all participants or their legal guardians.
Study population
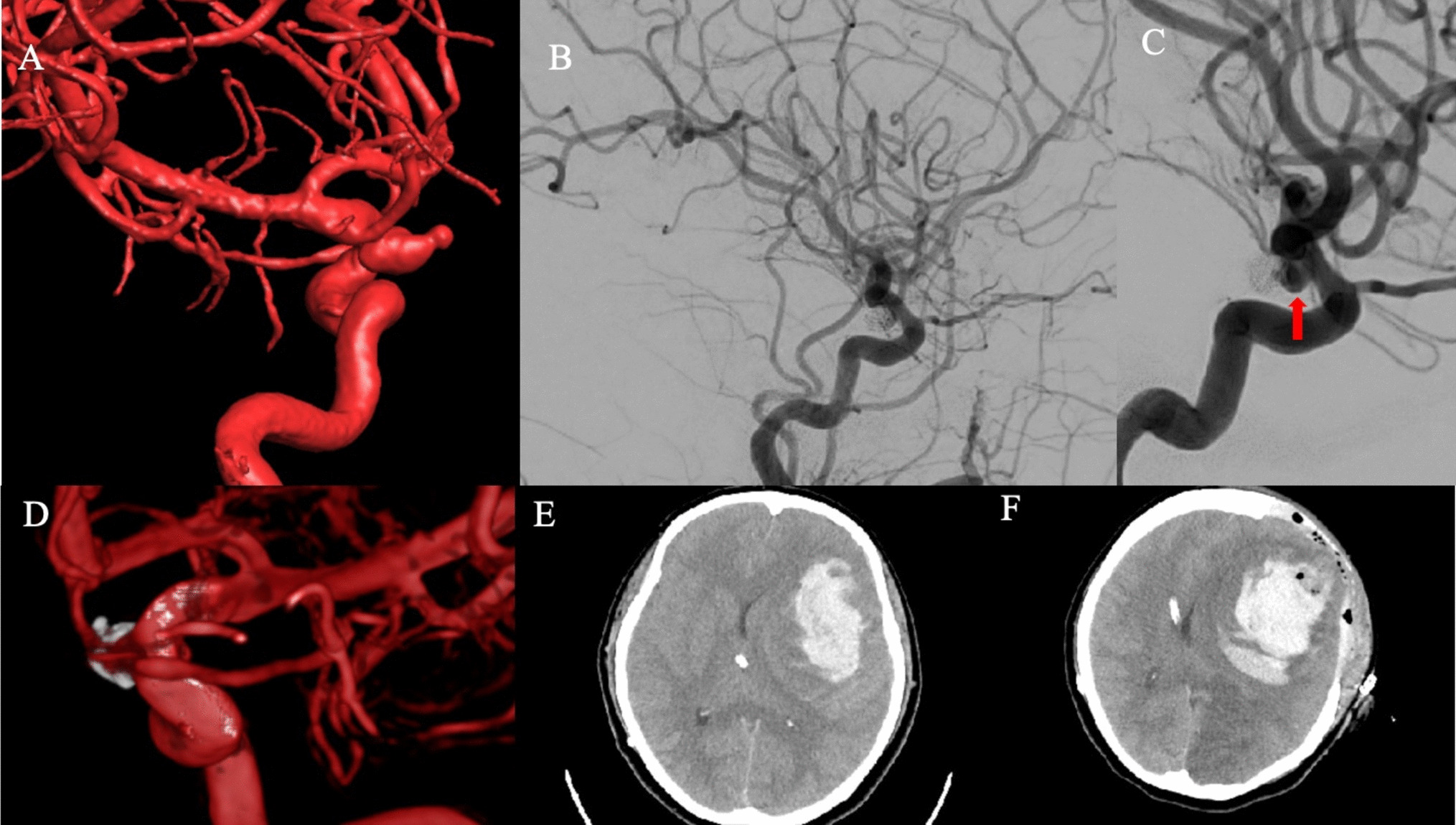
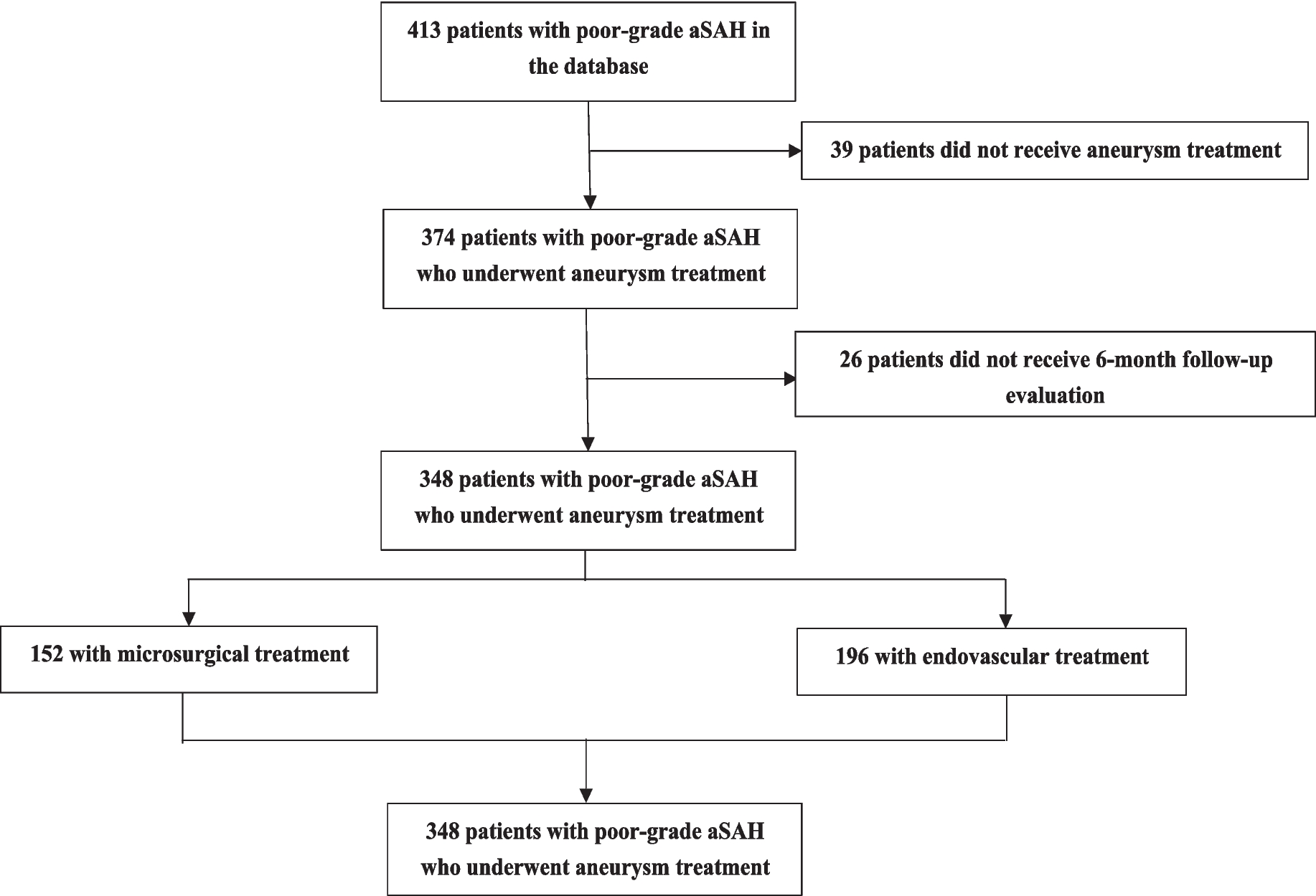
We identified patients with PGASAH through screening of our electronic medical database. Diagnosis of aSAH was made at admission based on computed tomography (CT) scans and/or lumbar puncture, demonstrating xanthochromic cerebrospinal fluid (CSF) indicative of subarachnoid blood, and proof of an intracranial aneurysm by angiogram. For the purposes of this study, clinical grade was recorded based on the patients' status at admission, prior to any interventions such as external ventricular drainage (EVD), medication, surgical treatment, or other therapeutic measures. Inclusion required patients aged ≥ 18 years who underwent aneurysm treatment in our neurosurgical department. Exclusion criteria included: 1) age < 18 years, 2) absence of aneurysm treatment, 3) lack of 6-month postoperative follow-up records.
Clinical therapeutic protocol
All patients admitted with suspected aSAH undergo radiographic imaging, including digital subtraction angiography (DSA) or CT angiography, to ascertain the source of bleeding. Treatment decisions, determined through collaborative assessments by the on-call neuroradiologist and neurosurgeon, involved microsurgical clipping or endovascular coiling. All patients received oral nimodipine for 21 days post-onset. Our treatment and management protocols strictly followed the international guidelines set forth by the American Heart Association/American Stroke Association (AHA/ASA) 2012 for the management of aSAH, ensuring standardized, evidence-based care for PGASAH patients [14].
For patients presenting with clinical or radiological evidence of elevated ICP (e.g., acute hydrocephalus, brain herniation, or severe neurological deterioration), ICP was monitored using EVD to ensure accurate measurements. Patients with clinical or radiological evidence of acute hydrocephalus underwent EVD insertion as part of standard management. For patients without EVD placement, ICP was assessed using radiological criteria, including compressed basal cisterns, midline shift, or significant ventricular dilation consistent with acute hydrocephalus. Patients with stable radiological dynamics were classified as having ICP ≤ 20 mmHg. Conservative treatment for ICP was initiated if ICP remained persistently elevated (> 20 mmHg), while decompressive craniectomy was considered for refractory cases. Transcranial Doppler ultrasound (TCD) was conducted daily for at least 14 days post-onset to identify cerebral vasospasm. Patients exhibiting clinical symptoms of vasospasm (TCD values > 120 m/s, new neurological deficit, or Glasgow Coma Scale (GCS) decline ≥ 2 points) were scheduled for DSA for verification and invasive endovascular treatment. Routine laboratory tests were conducted at admission and three times a week during stay on intensive care unit, with additional blood tests as necessary.
Additional routine CT scans were performed within the first 24 h post-treatment, after any further surgical interventions, or in case of clinical deterioration. Close monitoring of vital parameters in the intensive care unit or intermediate care unit was mandatory for at least 14 days post-aSAH.
Patient demographics and clinical parameters
Data on demographics, admission comorbidities, previous medication history, admission aSAH-related parameters, laboratory parameters, and complications during hospitalization were collected from electronic patient records, standardized admission protocols, and intensive care charts.
For statistical analysis, patients' age was dichotomized (≤ 55 years vs. > 55 years), corresponding to the cohort's median age. The size of the aneurysm sac was measured using DSA, and was categorized at a cutoff of 6 mm. Aneurysms exhibiting multiple lobes or irregular shapes were designated as "irregular aneurysm morphology." Initial clinical severity was quantified using the WFNS grading scale [15]. The extent of hemorrhage was assessed via the original Fisher scale [16], segregating severity into low (Fisher grades 1–2) and high (Fisher grades 3–4) categories.
Intracranial aneurysms are divided into anterior circulation aneurysms and posterior circulation aneurysms. Anterior circulation aneurysms include aneurysms that occur in a series of internal carotid artery systems, including the carotid artery, ophthalmic artery, choroidal artery, posterior communicating artery, middle cerebral artery, anterior cerebral artery, and anterior communicating artery. Posterior circulation aneurysms are aneurysms that occur in the vertebrobasilar artery, such as basilar artery aneurysms, posterior cerebral artery aneurysms, vertebral artery or superior cerebellar artery aneurysms, posterior cerebellar or anterior inferior cerebellar artery aneurysms. The incidences of both intracerebral (ICH) and intraventricular hemorrhages (IVH) were meticulously documented as well as laboratory parameters at admission.
Admission aSAH-related parameters included time from ictus to treatment (in days), Fisher grade 3–4, dilated pupil(s) at admission, and admission ICP > 20 mmHg. During statistical analysis, ICP values obtained via EVD were used as precise measurements, while radiological data were utilized for patients without invasive monitoring. For simplicity, ICP values were categorized dichotomously as either ≤ 20 mmHg or > 20 mmHg for statistical evaluation. Treatment modalities, including coiling or clipping, were documented, along with aneurysm location (anterior vs. posterior circulation), presence of IVH, ICH, and ICH evacuation. Additional parameters such as aneurysm size > 6 mm, multiple aneurysms, irregular aneurysm morphology, and admission maximum temperature (in Celsius) were also recorded.
Information regarding comorbidities such as obesity, drug abuse, alcohol abuse, hypercholesterolemia, diabetes, oncologic, hypothyroidism, hyperthyroidism, hyperuricemia/Gout, and cardiac valve disease, as well as previous medication history including beta blocker, calcium channel blocker, ACE inhibitor, AT1 antagonist, statin, acetylsalicylic acid (ASA), and warfarin, were extracted from patients' original medical records. Cardiac valve disease was defined as a history of clinically diagnosed valvular disease documented in the medical records or echocardiography findings, including valve stenosis, insufficiency, or other significant structural abnormalities. There were no patients with a history of valve replacement surgery in the final analysis.
We also recorded the complications during the acute hospitalization, including aneurysm rebleeding, CNS infection, decompressive craniectomy (DC), increased ICP, TCD > 120 m/s, angiographic vasospasm, systemic infection, sepsis, pneumonia, pleural effusion, pneumothorax, tracheotomy, bacteremia, acute coronary syndrome, new onset of arrhythmia, thrombotic complexes, gastrointestinal complication, liver dysfunction, epilepsy, seizure at onset (SaO), DCI infarction and early infarction. New low-density areas seen in follow-up CT scans, not attributable to surgical intervention or ICH, were classified as cerebral infarcts. Infarcts documented within 72 h post-hemorrhage were categorized as early infarctions [17], while those occurring subsequently were defined as delayed cerebral ischemia (DCI) [18].
Outcome
All outcomes were assessed by professional physicians using the modified Rankin Scale (mRS) [19] during the 6-month follow-up. The primary endpoint of this study was defined as an unfavorable outcome, characterized by an mRS score of 3 or higher at the 6-month follow-up. Functional disability was defined by mRS score ≥ 2. In-hospital mortality was documented.
Statistical analysis
Statistical analyses were conducted using SPSS Version 26 for Mac (IBM Corp.). The significance threshold was established at p < 0.05. If the count of missing values was less than 18, the complete-case analysis method was utilized, focusing solely on individuals with complete data across all variables. For counts equal to or exceeding 18, a univariate imputation approach was adopted. Categorical variables were imputed with mode values, while quantitative variables were imputed with means for analysis. Initially, a univariate analysis of all collected parameters was conducted to discern their impact on prognostic outcomes. Dichotomous variables were evaluated using Chi-square tests or Fisher's exact test for sample sizes less than five. Continuous variables were analyzed using Student's t-test for normally distributed data and the Mann–Whitney U test for non-normal distributions. Cut-off values for continuous variables were identified through receiver operating characteristic (ROC) curve analysis using the Youden index, aiming to maximize sensitivity and specificity. These thresholds were applied as criteria before inclusion in the multivariate analysis. Subsequently, significant variables (p < 0.05) from univariate analyses were incorporated into a multivariate binary logistic regression model to identify independent prognostic predictors. This multivariate analysis was executed in a staged approach: first, analyzing variables from premorbid conditions/medications, admission aSAH dependent/clinical parameters, admission laboratory parameters, and aSAH/clinical complications separately, and then integrating the significant variables from these analyses into the final multivariate model. Missing data were replaced using multiple imputation.
R version 4.3.0 (2023–04–21) was employed to construct prognostic nomograms integrating these independent risk factors. ROC curves were used to assess the discriminative ability of the nomograms. The area under the curve (AUC) represents the area covered by the ROC curve, with an AUC value approaching 1 indicating enhanced predictive efficacy. An AUC > 0.70 suggests acceptable model discrimination. Calibration curves were employed to assess the accuracy of the predictive model in estimating individual prognostic outcomes. Decision curve analysis (DCA) was utilized to evaluate the clinical utility of the prognostic model.


留言 (0)