
記住我
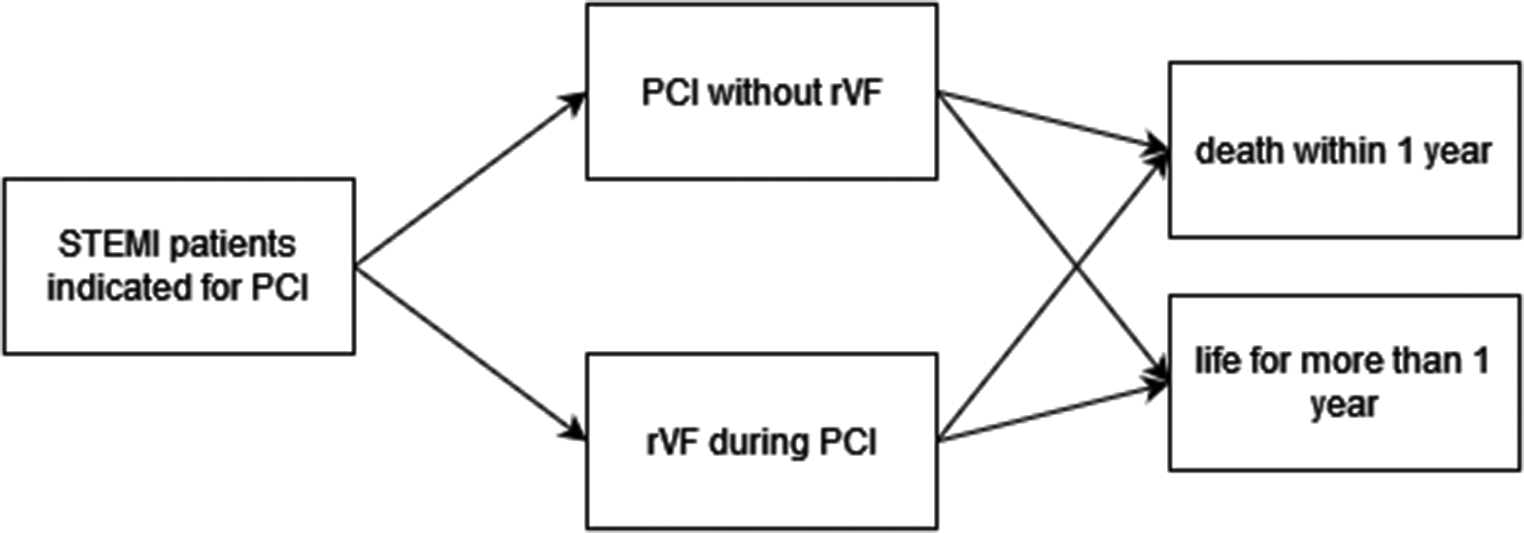






The Decision Tree Model was chosen for the modeling. The current model of STEMI patients indicated for PCI treatment and the model of using the new technology are compared. Figures 1 and 2 show simplified diagrams of existing (1) and new (2) technology.
Fig. 1
Model of current practice of STEMI patients indicated for PCI treatment. (Own analysis)
Fig. 2
Model of STEMI patients indicated for PCI treatment using new technology. (Own analysis)
The significant differences between the existing and new procedures are:
1.Advanced diagnostic of rVF risk predicted by the new procedure.
2.Medication of patients with diagnosed high risk of developing rVF during PCI in a new procedure.
Probabilities of transitions between individual model states were identified based on published basic research data and statistical data obtained from the literature (Table 1).
Table 1 Parameters of models related to clinical efficacy2.2 CostsAs part of the work, the costs associated with the use of new technology are viewed from the position of the health care payer. In the Czech Republic, health services are provided mainly on the basis of compulsory public health insurance, the payer being the health insurance company [27].
2.2.1 HospitalizationIn the Czech Republic, inpatient health care is reported and financed using the Diagnostic-Relational Groups (DRG) system. The DRG system is a methodology for classifying and funding hospitalizations that organizes patients into groups based on diagnostic and treatment characteristics. The aim is to ensure transparent and fair funding that meets the patient’s needs [28].
Each DRG group is assigned a weight or financial value that reflects the average cost associated with providing care to a patient in that category [29].
The model uses the average direct costs of hospitalization of STEMI patients undergoing PCI with and without rVF taken from the DRG-CZ database (Table 2) [30].
In order to calculate the total costs of using the new technology, it was necessary to determine and add the costs of additional staffing, instrumentation and material equipment associated with the use of the new technology to the known information about the costs of caring for STEMI patients undergoing PCI [31].
Table 2 Parameters of the cost modelsThe Czech Act no. 243/2021 was used to calculate personnel security costs. The maximum time for which the physician would spend determining the risk of rVF during PCI of STEMI patients by using the new evaluated technology was set for 5 min, including the possible prescription of medication in patients with an identified high risk of rVF during PCI. Although the process is also staffed by a professional administrative worker in the healthcare sector and, when medication is prescribed, nurses are also involved, but the DRG system already accounts for similar costs as part of standard hospitalization. Therefore, only the value of the doctor’s work beyond the standard examination is considered in the calculation [31].
The evaluated SW module is not yet available on the market and its price has been tentatively set at 20000 CZK (approx. 911 USD). The shelf life of the product is 5 years.
Based on data from the Ministry of Health Bulletin No. 13/2020, there are 18 centers of highly specialized cardiovascular care, which have their cardiocenter status valid until 31/12/2025 and are therefore authorized to perform PCI in the Czech Republic [32].
The premise of the financial analysis of the new concept of care for STEMI patients indicated for PCI is the installation of 2 SW licenses in each of the 18 cardiac centers in the Czech Republic. That’s a total of 36 licenses.
The Czech National Register of Cardiovascular Interventions provides data on performed PCIs through the Institute of Health Information and Statistics. The last available statistics of the register of cardiovascular interventions were compiled on 07.05.2023 and cover the period 2005–2021 [33].
From the published statistics for the last 5 years, on average around 5 910 PCIs are performed in STEMI patients in the Czech Republic [33]. This number of patients also form the basic cohort for calculation.
Centers for highly specialized cardiovascular care are evenly distributed across the territory of the Czech Republic, which is why their workloads are also relatively evenly distributed [32].
Therefore, the instrumentation cost calculation is calculated with 328 STEMI patients with an indication for PCI for each cardiac center per year. Each SW license for predicting the risk of rVF during PCI of STEMI patients will thus be used for the diagnosis of 164 patients per year.
The cost of using of the device for one diagnostic procedure will thus amount to 24.39 CZK (approx. 1.11 USD) (Table 2).
There are no cost items for consumables associated with the use of new technology, which will enable the examination of the risk of rVF during PCI of STEMI patients. However, the costs of consumables will arise in connection with any prescribed medication for STEMI patients with detected high risk of rVF during PCI.
Cost items and the amount of material consumed were determined based on consultations with cardiology center staff and only concern patients with high risk of rVF during PCI and indicated medication. In total, these costs will amount to 454.16 CZK (approx. 20.69 USD) for the melatonin medication of one STEMI patient with a diagnosed high risk of rVF during PCI (Table 2).
2.2.2 Pharmacologic therapy after hospital dischargeThe model also takes into account the costs of regular medication after the patient has been discharged from the hospital for a period of one year, which is also largely covered by the insurance company in the Czech Republic.
Basic medications after a heart attack include [34,35,36,37]:
Every post-myocardial infarction patient should have an ACE inhibitor, unless they have contraindications, and should take high doses (ramipril 10 mg, perindopril 8–10 mg, trandolapril 4 mg) if tolerated.
High doses of statins (atorvastatin or simvastatin 80 mg) are recommended)
Antiaggregation – the basis is acetylsalicylic acid in a dose of 75–360 mg (most often 100 mg in the Czech Republic), to which clopidogrel is added for several months (usually 12) after angioplasty or stenting.
Amiodarone 200 mg is additionally prescribed for patients after rVF.
The cost of monthly medication of STEMI patients after PCI was calculated on the basis of data from the database of the State Institute for Drug Control (SUKL). Core reimbursement from health insurance was considered (Table 2).
2.2.3 Modelling, scenarios, cost-effectiveness analysis and sensitivity analysisInformation and statistical data on clinical trials or patient studies about using of melatonin as rVF protector for STEMI patients have not yet been published, which is common for new developing technologies in healthcare. And therefore, within this eHTA study, scenarios for medication effectiveness (rate of rVF protection) of 5%, 10%, 20%, 30%, 40%, 50%, 60%, 70%, 80%, 90%, 95% were investigated.
Cost-effectiveness was evaluated by the CEA method, where the effect was calculated as the survival rate of the first year after STEMI solved by PCI. The simulations are carried out in the R. The ICER was calculated for individual scenarios and displayed on the incremental cost-effectiveness plane graph [38].
Furthermore, the minimum efficiency of rVF protecting medication to achieve the technology and procedure cost-effectiveness (intersection with the willingness-to-pay limit) and also the limit of efficiency of rVF protecting medication for transition to the “dominant intervention” state, when ∆C < 0 & ∆E > 0 (South-east [SE] quadrant), were determined [38].
For the sensitivity analysis, 2 scenarios were subsequently selected: the first according to the value of the minimum efficiency of rVF protecting medication for the intervention corresponding to the state of “dominant intervention” (when ∆C < 0 & ∆E > 0, South-east [SE] quadrant) and the second according to the mean value of the effectiveness of melatonin as rVF protector, which was proven in animal studies, i.e. 70% [38].
The sensitivity analysis was calculated with a margin of error for the probability values of rVF during PCI of STEMI patients, for mortality rates within 1 year, and also for the sensitivity and specificity of rVF prediction using the new technology. Hospitalization cost values were calculated with possible deviations of ± 30% and the effectiveness of medication with a deviation of ± 10% as part of the sensitivity analysis.
留言 (0)